REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
A vaginal fistula is an abnormal opening that connects your vagina to another organ, such as your bladder, colon or rectum. Your doctor might describe the condition as a hole in your vagina that allows stool or urine to pass through your vagina.
Vaginal fistulas can develop as a result of an injury, a surgery, an infection or radiation treatment. Whatever the cause of your fistula, you may need to have it closed by a surgeon to restore normal function.
There are several types of vaginal fistulas:
Vesicovaginal fistula. Also called a bladder fistula, this opening occurs between your vagina and urinary bladder and is the type that doctors see most often.
Ureterovaginal fistula. This type of fistula happens when the abnormal opening develops between your vagina and the ducts that carry urine from your kidneys to your bladder (ureters).
Urethrovaginal fistula. In this type of fistula, also called a urethral fistula, the opening occurs between your vagina and the tube that carries urine out of your body (urethra).
Rectovaginal fistula. In this type of fistula, the opening is between your vagina and the lower portion of your large intestine (rectum).
Colovaginal fistula. With a colovaginal fistula, the opening occurs between the vagina and colon.
Enterovaginal fistula. In this type of fistula, the opening is between the small intestine and the vagina
Vaginal Fistula Causes
Most often, the culprit is tissue damage because of things like:
Childbirth
Abdominal surgery (hysterectomy or cesarean section)
Pelvic, cervical, or colon cancer
Radiation treatment
Bowel disease like Crohn’s or diverticulitis
Infection (including after an episiotomy or a tear you had when you gave birth)
Traumatic injury, such as from a car accident
Vaginal Fistula Diagnosis
Your doctor will do a pelvic exam and ask about your medical history to see if you have any risk factors for fistulas, like a recent surgery, infection, or pelvic radiation.
They may also order some tests, including:
Dye test. Your doctor will fill your bladder with a dye solution. They’ll ask you to cough or bear down. If you have a vaginal fistula, the dye will leak into your vagina.
Cystoscopy. Your doctor uses a thin device called a cystoscope to look inside your bladder and urethra for signs of damage.
X-rays:
Retrograde pyelogram. This is a special test in which dye is injected through your bladder into your ureters. An X-ray can show whether there is leakage between a ureter and your vagina.
Fistulogram. This is an X-ray image of your fistula. It can show your doctor whether you have one or many fistulas and if other pelvic organs may be involved.
Flexible sigmoidoscopy. Your doctor looks at your anus and rectum with a sigmoidoscope (a thin, flexible tube with a tiny video camera at the tip).
CT urogram. You have dye injected into a vein, and CT scans make images of your vagina and urinary tract.
Pelvic MRI. A magnetic field and radio waves take detailed pictures of your rectum and vagina to help show the details of a rectovaginal fistula.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Vaginal Fistula Symptoms
A vaginal fistula doesn’t usually hurt, but it can cause some problems that need medical care. If you have a vesicovaginal fistula (an opening between your vagina and bladder), urine will constantly leak from your bladder into your vagina. This can make you unable to control your urination (incontinent).
Also, your genital area may get infected or sore, and you can have pain during intercourse.
Other symptoms of vaginal fistulas include:
Fever
Belly pain
Diarrhea
Weight loss
Nausea
Vomiting
Vaginal Fistula Complications
Vaginal fistulas can be upsetting and embarrassing when they leak and cause bad smells. But they can also cause complications like:
Vaginal or urinary tract infections that keep coming back
Hygiene problems
Stool or gas that leaks through the vagina
Irritated or inflamed skin around your vagina or anus
A swollen clump of infected tissue with pus (abscess) that could be dangerous without treatment
Fistulas that come back
Women who have Crohn’s disease and develop a fistula have a high risk of complications, such as fistulas forming again later or fistulas that don’t properly heal.
Vaginal Fistula Treatment
Some fistulas may heal on their own. If it’s a small bladder fistula, your doctor might want to try putting a small tube called a catheter into your bladder to drain the pee and give the fistula time to heal by itself.
They might also use a special glue or plug made of natural proteins to seal or fill the fistula. They can also give you an antibiotic to treat an infection caused by the fistula.
Many people who have fistulas need surgery. What kind of surgery you get depends on the type of fistula and where it is. It could be laparoscopic, in which your doctor makes small cuts (incisions) and inserts cameras and tools. Or it could be abdominal surgery, where you get a regular incision with a tool called a scalpel.
For a vaginal fistula that connects to your rectum, your doctor might:
Sew a special patch over the fistula
Take tissue from another place in your body to close it
Fold a flap of healthy tissue over the fistula
Fix the muscles of your anus if they’re damaged
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Gestational trophoblastic disease (GTD) can be benign or malignant. Histologically, it is classified into hydatidiform mole, invasive mole (chorioadenoma destruens), choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor (ETT). Those that invade locally or metastasize are collectively known as gestational trophoblastic neoplasia (GTN). Hydatidiform mole is the most common form of GTN. While invasive mole and choriocarcinoma are malignant, a hydatidiform mole can behave in a malignant or benign fashion.
No methods exist to accurately predict the clinical behavior of a hydatidiform mole by histopathology. The clinical course is defined by the patient’s serum human chorionic gonadotropin (hCG) curve after evacuation of the mole. In 80% of patients with a benign hydatidiform mole, serum hCG levels steadily drop to normal within 8-12 weeks after evacuation of the molar pregnancy. In the other 20% of patients with a malignant hydatidiform mole, serum hCG levels either rise or plateau.
The International Federation of Gynecology and Obstetrics considers an elevated serum hCG level 6 or more months after evacuation of a hydatidiform mole to be diagnostic of malignancy (ie, GTN). However, serum hCG levels spontaneously return to normal without chemotherapy in most patients with elevated but still declining serum hCG levels 6 months after diagnosis of a hydatidiform mole. Therefore, continuing to follow these patients is reasonable as long as the hCG levels do not rise or plateau.
United States
Gestational trophoblastic neoplasia is diagnosed in 15-20% of patients with a complete hydatidiform mole and 2% of partial hydatidiform moles. Lung metastases are found in 4-5% of patients with complete hydatidiform moles and rarely in cases of partial hydatidiform moles.
Choriocarcinoma occurs in 1 out of 40 hydatidiform moles and in 1 out of 20,000-40,000 pregnancies.However, only 1 out of 160,000 term pregnancies is followed by a choriocarcinoma.
International
The international rate of choriocarcinoma has been reported to be as high as 1 in 500-600 pregnancies in India to 1 in 50,000 pregnancies in Mexico, Paraguay, and Sweden.These differences are probably due to differences in methodology (eg, identification of cases, accuracy of denominator).
Race-, sex-, age-related demographics
Little information is available on international ethnic or racial differences of the incidence of choriocarcinoma. In the United States, African Americans have the highest incidence of choriocarcinoma and the lowest survival rates.
Gestational trophoblastic neoplasia affects women during their reproductive years. However, placental site trophoblastic tumors have been diagnosed when patients were postmenopausal.
The incidence of choriocarcinoma increases with age and is 5-15 times higher in women 40 years and older than in younger women.
Gestational trophoblastic disease (GTD) is a group of rare diseases in which abnormal trophoblast cells grow inside the uterus after conception.
In gestational trophoblastic disease (GTD), a tumor develops inside the uterus from tissue that forms after conception (the joining of sperm and egg). This tissue is made of trophoblast cells and normally surrounds the fertilized egg in the uterus. Trophoblast cells help connect the fertilized egg to the wall of the uterus and form part of the placenta (the organ that passes nutrients from the mother to the fetus).
Sometimes there is a problem with the fertilized egg and trophoblast cells. Instead of a healthy fetus developing, a tumor forms. Until there are signs or symptoms of the tumor, the pregnancy will seem like a normal pregnancy.
Most GTD is benign (not cancer) and does not spread, but some types become malignant (cancer) and spread to nearby tissues or distant parts of the body.
Gestational trophoblastic disease (GTD) is a general term that includes different types of disease:
Hydatidiform Moles (HM)
Complete HM.
Partial HM.
Gestational Trophoblastic Neoplasia (GTN)
Invasive moles.
Choriocarcinomas.
Placental-site trophoblastic tumors (PSTT; very rare).
Epithelioid trophoblastic tumors (ETT; even more rare).
Hydatidiform mole (HM) is the most common type of GTD.
HMs are slow-growing tumors that look like sacs of fluid. An HM is also called a molar pregnancy. The cause of hydatidiform moles is not known.
HMs may be complete or partial:
A complete HM forms when sperm fertilizes an egg that does not contain the mother’s DNA. The egg has DNA from the father and the cells that were meant to become the placenta are abnormal.
A partial HM forms when sperm fertilizes a normal egg and there are two sets of DNA from the father in the fertilized egg. Only part of the fetus forms and the cells that were meant to become the placenta are abnormal.
Most hydatidiform moles are benign, but they sometimes become cancer. Having one or more of the following risk factors increases the risk that a hydatidiform mole will become cancer:
A pregnancy before 20 or after 35 years of age.
A very high level of beta human chorionic gonadotropin (β-hCG), a hormone made by the body during pregnancy.
A large tumor in the uterus.
An ovarian cyst larger than 6 centimeters.
High blood pressure during pregnancy.
An overactive thyroid gland (extra thyroid hormone is made).
Severe nausea and vomiting during pregnancy.
Trophoblastic cells in the blood, which may block small blood vessels.
Serious blood clotting problems caused by the HM.
Gestational trophoblastic neoplasia (GTN) is a type of gestational trophoblastic disease (GTD) that is almost always malignant.
Gestational trophoblastic neoplasia (GTN) includes the following:
Invasive moles
Invasive moles are made up of trophoblast cells that grow into the muscle layer of the uterus. Invasive moles are more likely to grow and spread than a hydatidiform mole. Rarely, a complete or partial HM may become an invasive mole. Sometimes an invasive mole will disappear without treatment.
Choriocarcinomas
A choriocarcinoma is a malignant tumor that forms from trophoblast cells and spreads to the muscle layer of the uterus and nearby blood vessels. It may also spread to other parts of the body, such as the brain, lungs, liver, kidney, spleen, intestines, pelvis, or vagina. A choriocarcinoma is more likely to form in women who have had any of the following:
Molar pregnancy, especially with a complete hydatidiform mole.
Normal pregnancy.
Tubal pregnancy (the fertilized egg implants in the fallopian tube rather than the uterus).
Miscarriage.
Placental-site trophoblastic tumors
A placental-site trophoblastic tumor (PSTT) is a rare type of gestational trophoblastic neoplasia that forms where the placenta attaches to the uterus. The tumor forms from trophoblast cells and spreads into the muscle of the uterus and into blood vessels. It may also spread to the lungs, pelvis, or lymph nodes. A PSTT grows very slowly and signs or symptoms may appear months or years after a normal pregnancy.
Epithelioid trophoblastic tumors
An epithelioid trophoblastic tumor (ETT) is a very rare type of gestational trophoblastic neoplasia that may be benign or malignant. When the tumor is malignant, it may spread to the lungs.
Age and a previous molar pregnancy affect the risk of GTD.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk to your doctor if you think you may be at risk. Risk factors for GTD include the following:
Being pregnant when you are younger than 20 or older than 35 years of age.
Having a personal history of hydatidiform mole.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Signs of GTD include abnormal vaginal bleeding and a uterus that is larger than normal.
These and other signs and symptoms may be caused by gestational trophoblastic disease or by other conditions. Check with your doctor if you have any of the following:
Vaginal bleeding not related to menstruation.
A uterus that is larger than expected during pregnancy.
Pain or pressure in the pelvis.
Severe nausea and vomiting during pregnancy.
High blood pressure with headache and swelling of feet and hands early in the pregnancy.
Vaginal bleeding that continues for longer than normal after delivery.
Fatigue, shortness of breath, dizziness, and a fast or irregular heartbeat caused by anemia.
GTD sometimes causes an overactive thyroid. Signs and symptoms of an overactive thyroid include the following:
Fast or irregular heartbeat.
Shakiness.
Sweating.
Frequent bowel movements.
Trouble sleeping.
Feeling anxious or irritable.
Weight loss.
Tests that examine the uterus are used to detect (find) and diagnose gestational trophoblastic disease.
The following tests and procedures may be used:
Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
Pelvic exam: An exam of the vagina, cervix, uterus, fallopian tubes, ovaries, and rectum. A speculum is inserted into the vagina and the doctor or nurse looks at the vagina and cervix for signs of disease. A Pap test of the cervix is usually done. The doctor or nurse also inserts one or two lubricated, gloved fingers of one hand into the vagina and places the other hand over the lower abdomen to feel the size, shape, and position of the uterus and ovaries. The doctor or nurse also inserts a lubricated, gloved finger into the rectum to feel for lumps or abnormal areas.EnlargePelvic exam. A doctor or nurse inserts one or two lubricated, gloved fingers of one hand into the vagina and presses on the lower abdomen with the other hand. This is done to feel the size, shape, and position of the uterus and ovaries. The vagina, cervix, fallopian tubes, and rectum are also checked.
Ultrasound exam of the pelvis: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs in the pelvis and make echoes. The echoes form a picture of body tissues called a sonogram. Sometimes a transvaginal ultrasound (TVUS) will be done. For TVUS, an ultrasound transducer (probe) is inserted into the vagina to make the sonogram.
Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease. Blood is also tested to check the liver, kidney, and bone marrow.
Serum tumor marker test: A procedure in which a sample of blood is checked to measure the amounts of certain substances made by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the body. These are called tumor markers. For GTD, the blood is checked for the level of beta human chorionic gonadotropin (β-hCG), a hormone that is made by the body during pregnancy. β-hCG in the blood of a woman who is not pregnant may be a sign of GTD.
Urinalysis: A test to check the color of urine and its contents, such as sugar, protein, blood, bacteria, and the level of β-hCG.
Certain factors affect prognosis (chance of recovery) and treatment options.
Gestational trophoblastic disease usually can be cured. Treatment and prognosis depend on the following:
The type of GTD.
Whether the tumor has spread to the uterus, lymph nodes, or distant parts of the body.
The number of tumors and where they are in the body.
The size of the largest tumor.
The level of β-hCG in the blood.
How soon the tumor was diagnosed after the pregnancy began.
Whether GTD occurred after a molar pregnancy, miscarriage, or normal pregnancy.
Previous treatment for gestational trophoblastic neoplasia.
Treatment options also depend on whether the woman wishes to become pregnant in the future.
Stages of Gestational Trophoblastic Tumors and Neoplasia
Key Points
After gestational trophoblastic neoplasia has been diagnosed, tests are done to find out if cancer has spread from where it started to other parts of the body.
There are three ways that cancer spreads in the body.
Cancer may spread from where it began to other parts of the body.
There is no staging system for hydatidiform moles.
The following stages are used for GTN:
Stage I
Stage II
Stage III
Stage IV
The treatment of gestational trophoblastic neoplasia is based on the type of disease, stage, or risk group.
After gestational trophoblastic neoplasia has been diagnosed, tests are done to find out if cancer has spread from where it started to other parts of the body.
The process used to find out the extent or spread of cancer is called staging, The information gathered from the staging process helps determine the stage of disease. For GTN, stage is one of the factors used to plan treatment.
The following tests and procedures may be done to help find out the stage of the disease:
Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body onto film, making pictures of areas inside the body.
CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
MRI (magnetic resonance imaging) with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as brain and spinal cord. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Lumbar puncture: A procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs that the cancer has spread to the brain and spinal cord. This procedure is also called an LP or spinal tap.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
Tissue. The cancer spreads from where it began by growing into nearby areas.
Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if choriocarcinoma spreads to the lung, the cancer cells in the lung are actually choriocarcinoma cells. The disease is metastatic choriocarcinoma, not lung cancer.
There is no staging system for hydatidiform moles.
Hydatidiform moles (HM) are found in the uterus only and do not spread to other parts of the body.
The following stages are used for GTN:
Stage I
In stage I, the tumor is in the uterus only.
Stage II
In stage II, cancer has spread outside of the uterus to the ovary, fallopian tube, vagina, and/or the ligaments that support the uterus.
Stage III
In stage III, cancer has spread to the lung.
Stage IV
In stage IV, cancer has spread to distant parts of the body other than the lungs.
The treatment of gestational trophoblastic neoplasia is based on the type of disease, stage, or risk group.
Invasive moles and choriocarcinomas are treated based on risk groups. The stage of the invasive mole or choriocarcinoma is one factor used to determine risk group. Other factors include the following:
The age of the patient when the diagnosis is made.
Whether the GTN occurred after a molar pregnancy, miscarriage, or normal pregnancy.
How soon the tumor was diagnosed after the pregnancy began.
The level of beta human chorionic gonadotropin (β-hCG) in the blood.
The size of the largest tumor.
Where the tumor has spread to and the number of tumors in the body.
How many chemotherapy drugs the tumor has been treated with (for recurrent or resistant tumors).
There are two risk groups for invasive moles and choriocarcinomas: low risk and high risk. Patients with low-risk disease usually receive less aggressive treatment than patients with high-risk disease.
Placental-site trophoblastic tumor (PSTT) and epithelioid trophoblastic tumor (ETT) treatments depend on the stage of disease.
Recurrent and Resistant Gestational Trophoblastic Neoplasia
Recurrent gestational trophoblastic neoplasia (GTN) is cancer that has recurred (come back) after it has been treated. The cancer may come back in the uterus or in other parts of the body.
Gestational trophoblastic neoplasia that does not respond to treatment is called resistant GTN.
Treatment Option Overview
Key Points
There are different types of treatment for patients with gestational trophoblastic disease.
Three types of standard treatment are used:
Surgery
Chemotherapy
Radiation therapy
New types of treatment are being tested in clinical trials.
Treatment for gestational trophoblastic disease may cause side effects.
Patients may want to think about taking part in a clinical trial.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Follow-up tests may be needed.
There are different types of treatment for patients with gestational trophoblastic disease.
Different types of treatment are available for patients with gestational trophoblastic disease. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. Before starting treatment, patients may want to think about taking part in a clinical trial. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Clinical trials are taking place in many parts of the country. Information about ongoing clinical trials is available from the NCI website. Choosing the most appropriate cancer treatment is a decision that ideally involves the patient, family, and health care team.
Three types of standard treatment are used:
Surgery
The doctor may remove the cancer using one of the following operations:
Dilatation and curettage (D&C) with suction evacuation: A surgical procedure to remove abnormal tissue and parts of the inner lining of the uterus. The cervix is dilated and the material inside the uterus is removed with a small vacuum-like device. The walls of the uterus are then gently scraped with a curette (spoon-shaped instrument) to remove any material that may remain in the uterus. This procedure may be used for molar pregnancies.EnlargeDilatation and curettage (D and C). A speculum is inserted into the vagina to widen it in order to look at the cervix (first panel). A dilator is used to widen the cervix (middle panel). A curette is put through the cervix into the uterus to scrape out abnormal tissue (last panel).
Hysterectomy: Surgery to remove the uterus, and sometimes the cervix. If the uterus and cervix are taken out through the vagina, the operation is called a vaginal hysterectomy. If the uterus and cervix are taken out through a large incision (cut) in the abdomen, the operation is called a total abdominal hysterectomy. If the uterus and cervix are taken out through a small incision (cut) in the abdomen using a laparoscope, the operation is called a total laparoscopic hysterectomy.EnlargeHysterectomy. The uterus is surgically removed with or without other organs or tissues. In a total hysterectomy, the uterus and cervix are removed. In a total hysterectomy with salpingo-oophorectomy, (a) the uterus plus one (unilateral) ovary and fallopian tube are removed; or (b) the uterus plus both (bilateral) ovaries and fallopian tubes are removed. In a radical hysterectomy, the uterus, cervix, both ovaries, both fallopian tubes, and nearby tissue are removed. These procedures are done using a low transverse incision or a vertical incision.
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated, or whether the tumor is low-risk or high-risk.
Combination chemotherapy is treatment using more than one anticancer drug.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
External radiation therapy uses a machine outside the body to send radiation toward the cancer.
Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type of gestational trophoblastic disease being treated. External radiation therapy is used to treat gestational trophoblastic disease.
New types of treatment are being tested in clinical trials.
Information about ongoing clinical trials is available from the NCI website.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Blood levels of beta human chorionic gonadotropin (β-hCG) will be checked for up to 6 months after treatment has ended. This is because a β-hCG level that is higher than normal may mean that the tumor has not responded to treatment or it has become cancer.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Vaginal discharge is most often a normal and regular occurrence. However, there are certain types of discharge that can indicate an infection. Abnormal discharge may be yellow or green, chunky in consistency, or foul smelling.
Yeast or a bacterial infection usually causes abnormal discharge. If you notice any discharge that looks unusual or smells foul, see your doctor for diagnosis and treatment.
Types of vaginal discharge
There are several different types of vaginal discharge. These types are categorized based on their color and consistency. Some types of discharge are normal. Others may indicate an underlying condition that requires treatment.
White
A bit of white discharge, especially at the beginning or end of your menstrual cycle, is normal. However, if the discharge is accompanied by itching and has a thick, cottage cheese-like consistency or appearance, it’s not normal and needs treatment. This type of discharge may be a sign of a yeast infection.
Clear and watery
A clear and watery discharge is perfectly normal. It can occur at any time of the month. It may be especially heavy after exercise.
Clear and stretchy
When discharge is clear but stretchy and mucous-like, rather than watery, it indicates that you are likely ovulating. This is a normal type of discharge.
Brown or bloody
Brown or bloody discharge is usually normal, especially when it occurs during or right after your menstrual cycle. A late discharge at the end of your period can look brown instead of red. You may also experience a small amount of bloody discharge between periods. This is called spotting.
If spotting occurs during the normal time of your period and you’ve recently had sex without protection, this could be a sign of pregnancy. Spotting during an early phase of pregnancy can be a sign of miscarriage, so it should be discussed with your OB-GYN.
In rare cases, brown or bloody discharge can be a sign of endometrial or cervical cancer. It could be other problems such as fibroids or other abnormal growths. This is why it’s important to get a yearly pelvic exam and Pap smear. Your gynecologist will check for cervical abnormalities during these procedures.
Yellow or green
A yellow or green discharge, especially when it’s thick, chunky, or accompanied by an unpleasant smell, isn’t normal. This type of discharge may be a sign of the infection trichomoniasis. It’s commonly spread through sexual intercourse.
Causes of vaginal discharge
Normal vaginal discharge is a healthy bodily function. It’s your body’s way of cleaning and protecting the vagina. For instance, it’s normal for discharge to increase with sexual arousal and ovulation. Exercise, use of birth control pills, and emotional stress may also result in discharge.
Abnormal vaginal discharge, however, is usually caused by an infection.
Bacterial vaginosis
Bacterial vaginosis is a quite common bacterial infection. It causes increased vaginal discharge that has a strong, foul, and sometimes fishy odor, although it produces no symptoms in some cases. Women who receive oral sex or who have multiple sexual partners have an increased risk of acquiring this infection.
Trichomoniasis
Trichomoniasis is another type of infection. It’s caused by a protozoan, or single-celled organism. The infection is usually spread by sexual contact, but it can also be contracted by sharing towels or bathing suits. It results in a yellow or green discharge that has a foul odor. Pain, inflammation, and itching are also common symptoms, although some people don’t experience any symptoms.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Yeast infection
A yeast infection is a fungal infection that produces white, cottage cheese-like discharge in addition to burning and itching sensations. The presence of yeast in the vagina is normal, but its growth can multiply out of control in certain situations. The following may increase your likelihood of yeast infections:
stress
diabetes
use of birth control pills
pregnancy
antibiotics, especially prolonged use over 10 days
Gonorrhea and chlamydia
Gonorrhea and chlamydia are sexually transmitted infections (STIs) that can produce an abnormal discharge. It’s often yellow, greenish, or cloudy in color.
Pelvic inflammatory disease (PID)
Pelvic inflammatory disease (PID) is an infection that’s often spread by sexual contact. It occurs when bacteria spread up the vagina and into other reproductive organs. It may produce a heavy, foul-smelling discharge.
Human papillomavirus (HPV) or cervical cancer
The human papillomavirus (HPV) infection is spread by sexual contact. It can lead to cervical cancer. While there may be no symptoms, this type of cancer can produce a bloody, brown, or watery discharge with an unpleasant odor. Cervical cancer can easily be screened for with yearly Pap smears and HPV testingTrusted Source.
When to seek medical help
If you have unusual discharge alongside certain other symptoms, see your doctor as soon as possible. The symptoms to watch out for include:
fever
pain in the abdomen
unexplained weight loss
fatigue
increased urination
If you have any concerns regarding whether a discharge is normal, make an appointment to see your doctor.
What to expect at a doctor’s appointment
When you see your doctor for abnormal vaginal discharge, you’ll get a physical exam, including a pelvic exam. Your doctor will also ask you several questions about your symptoms, your menstrual cycle, and your sexual activity. In many cases, an infection can be detected by the physical or pelvic exam.
If your doctor can’t diagnose the problem immediately, they may order some tests. Your doctor may want to take a scraping from your cervix to check for HPV or cervical cancer. Your discharge may also be examined under a microscope to pinpoint an infectious agent. Once your doctor can tell you the cause of the discharge, you’ll be given treatment options.
Home care for vaginal discharge
To prevent infections, practice good hygiene and wear breathable cotton underwear. Don’t use douches, as they can make discharge worse by removing useful bacteria. Also, practice safe sex and use protection to avoid STIs.
To decrease the likelihood of yeast infections when taking antibiotics, eat yogurt that contains live and active cultures. If you know you have a yeast infection, you can also treat it with an over-the-counter yeast infection cream or suppository.
How is abnormal discharge treated?
How you are treated will depend on what’s causing the problem. For example, yeast infections are usually treated with antifungal medications inserted into the vagina in cream or gel form. Bacterial vaginosis is treated with antibiotic pills or creams. Trichomoniasis is usually treated with the drug metronidazole (Flagyl) or tinidazole (Tindamax).
Here are some tips for preventing vaginal infections that can lead to abnormal discharge:
Keep the vagina clean by washing with a gentle, mild soap and warm water on the outside. There is no need to put soap directly in the vagina.
Never use scented soaps and feminine products or douche. Also avoid feminine sprays and bubble baths.
After going to the bathroom, always wipe from front to back to prevent bacteria from getting into the vagina and causing an infection.
Wear 100% cotton underpants, and avoid overly tight clothing
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
STIs and STDs in women
Sexually transmitted infections and diseases (STIs and STDs) are transmitted through vaginal, anal, or oral sexual contact. Symptoms of an STD for those with a vagina can include:
vaginal itching
rashes
unusual discharge
pain
Many STIs display no symptoms at all. Left untreated, they can lead to fertility problems and an increased risk of cervical cancer. These risks make it even more important to practice safer sex.
Every year worldwide, there are approximately 376 millionTrusted Source new transmissions of syphilis, chlamydia, gonorrhea, and trichomoniasis.
Because many people with vaginas don’t show symptoms with some STIs, they may not know they need treatment. It’s estimated that as many as 1 in 6 Americans has genital herpes, but most are unawareTrusted Source that they have it.
Common STIs in women
Some of the most common STIs in women and those with a vagina include:
human papillomavirus (HPV)
gonorrhea
chlamydia
genital herpes
HPV is the most common STI in women. It’s also the main cause of cervical cancer.
A vaccine is available that can help prevent certain strains of HPV up to age 45 yearsTrusted Source. For more information, read about the pros and cons of the HPV vaccine.
Gonorrhea and chlamydia are common bacterial STIs. In fact, chlamydia is the most commonly reported STI in the Unites States.
Some gynecologists will automatically check for both during normal checkups, but you should ask for medical screening if you think you may be at risk.
Genital herpes is also common, with about 1 out of 6Trusted Source people between the ages 14 and 49 years having it.
Common symptoms of STIs
Women should be aware of possible STI symptoms so that they can seek medical advice if necessary. Some of the most common symptoms are described below.
Changes in urination. An STI can be indicated by pain or a burning sensation during urination, the need to pee more frequently, or the presence of blood in the urine.
Abnormal vaginal discharge. The look and consistency of vaginal discharge changes continually through a woman’s cycle or even in the absence of a cycle. Thick, white discharge can be a sign of a yeast infection. When discharge is yellow or green, it might indicate gonorrhea or trichomoniasis.
Itching in the vaginal area. Itching is a nonspecific symptom that may or may not be related to an STI. Sex-related causes for vaginal itching may include:
allergic reaction to a latex condom
yeast infection
pubic lice or scabies
genital warts
the early phases of most bacterial and viral STIs
Pain during sex. This symptom is often overlooked, but abdominal or pelvic pain can be a sign of pelvic inflammatory disease (PID). PID is most commonly caused by the advanced stage of chlamydia or gonorrhea.
Abnormal bleeding. Abnormal bleeding is another possible sign of PID or other reproductive problems cause by an STI.
Rashes or sores. Sores or tiny pimples around the mouth or vagina can indicate herpes, HPV, or syphilis.
f you have sex — oral, anal or vaginal intercourse and genital touching — you can get an STD, also called a sexually transmitted infection (STI). Regardless of your marital status or sexual orientation, you’re vulnerable to STIs and STI symptoms. Thinking or hoping your partner doesn’t have an STI is no protection — you need to know for sure.
Condoms, when properly used, are highly effective for reducing transmission of some STDs. But no method is foolproof, and STI symptoms aren’t always obvious. If you think you have STI symptoms or have been exposed to an STI, see a doctor. Also, inform your partner or partners so that they can be evaluated and treated.
Some STIs are easy to treat and cure; others require more-complicated treatment to manage them.
If untreated, STIs can increase your risk of acquiring another STI such as HIV. This happens because an STI can stimulate an immune response in the genital area or cause sores, either of which might raise the risk of HIV transmission. Some untreated STIs can also lead to infertility, organ damage, certain types of cancer or death.
Asymptomatic STIs
Many STIs have no signs or symptoms (asymptomatic). Even with no symptoms, however, you can pass the infection to your sex partners. So it’s important to use protection, such as a condom, during sex. And visit your doctor regularly for STI screening so you can identify and treat an infection before you can pass it on.
Chlamydia symptoms
Chlamydia is a bacterial infection of your genital tract. Chlamydia may be difficult to detect because early-stage infections often cause few or no signs and symptoms. When they do occur, symptoms usually start one to three weeks after you’ve been exposed to chlamydia and may be mild and pass quickly.
Signs and symptoms may include:
Painful urination
Lower abdominal pain
Vaginal discharge in women
Discharge from the penis in men
Pain during sexual intercourse in women
Bleeding between periods in women
Testicular pain in men
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Gonorrhea symptoms
Gonorrhea is a bacterial infection of your genital tract. The bacteria can also grow in your mouth, throat, eyes and anus. The first gonorrhea symptoms generally appear within 10 days after exposure. However, some people may be infected for months before signs or symptoms occur.
Signs and symptoms of gonorrhea may include:
Thick, cloudy or bloody discharge from the penis or vagina
Pain or burning sensation when urinating
Heavy menstrual bleeding or bleeding between periods
Painful, swollen testicles
Painful bowel movements
Anal itching
Trichomoniasis symptoms
Trichomoniasis is a common STI caused by a microscopic, one-celled parasite called Trichomonas vaginalis. This organism spreads during sexual intercourse with someone who already has the infection.
The organism usually infects the urinary tract in men, but often causes no symptoms. Trichomoniasis typically infects the vagina in women. When trichomoniasis causes symptoms, they may appear within five to 28 days of exposure and range from mild irritation to severe inflammation.
Signs and symptoms may include:
Clear, white, greenish or yellowish vaginal discharge
Discharge from the penis
Strong vaginal odor
Vaginal itching or irritation
Itching or irritation inside the penis
Pain during sexual intercourse
Painful urination
HIV symptoms
HIV is an infection with the human immunodeficiency virus. HIV interferes with your body’s ability to fight off viruses, bacteria and fungi that cause illness, and it can lead to AIDS, a chronic, life-threatening disease.
When first infected with HIV, you may have no symptoms. Some people develop a flu-like illness, usually two to six weeks after being infected. Still, the only way you know if you have HIV is to be tested.
Early signs and symptoms
Early HIV signs and symptoms usually disappear within a week to a month and are often mistaken for those of another viral infection. During this period, you’re highly infectious. More-persistent or -severe symptoms of HIV infection may not appear for 10 years or more after the initial infection. Early-stage HIV symptoms may include:
Fever
Headache
Sore throat
Swollen lymph glands
Rash
Fatigue
As the virus continues to multiply and destroy immune cells, you may develop mild infections or chronic signs and symptoms such as:
Swollen lymph nodes — often one of the first signs of HIV infection
Diarrhea
Weight loss
Fever
Cough and shortness of breath
Late-stage HIV infection
Signs and symptoms of late-stage HIV infection include:
Persistent, unexplained fatigue
Soaking night sweats
Shaking chills or fever higher than 100.4 F (38 C) for several weeks
Swelling of lymph nodes for more than three months
Chronic diarrhea
Persistent headaches
Unusual, opportunistic infections
Genital herpes symptoms
Genital herpes is a highly contagious STI caused by a type of the herpes simplex virus (HSV) that enters your body through small breaks in your skin or mucous membranes. Most people with HSV never know they have it, because they have no signs or symptoms or the signs and symptoms are so mild they go unnoticed.
When signs and symptoms are noticeable, the first episode is generally the worst. Some people never have a second episode. Others, however, can have recurrent episodes for decades.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
When present, genital herpes signs and symptoms may include:
Small red bumps, blisters (vesicles) or open sores (ulcers) in the genital and anal areas and areas nearby
Pain or itching around the genital area, buttocks and inner thighs
Ulcers can make urination painful. You may also have pain and tenderness in your genital area until the infection clears. During an initial episode, you may have flu-like signs and symptoms, such as a headache, muscle aches and fever, as well as swollen lymph nodes in your groin.
In some cases, the infection can be active and contagious even when sores aren’t present.
Human papillomavirus (HPV) infection and genital warts symptoms
HPV infection is one of the most common types of STIs. Some forms of HPV put women at high risk of cervical cancer. Other forms cause genital warts. HPV usually has no signs or symptoms. The signs and symptoms of genital warts include:
Small, flesh-colored or gray swellings in your genital area
Several warts close together that take on a cauliflower shape
Itching or discomfort in your genital area
Bleeding with intercourse
Often, however, genital warts cause no symptoms. Genital warts may be as small as 1 millimeter in diameter or may multiply into large clusters. Warts can also develop in the mouth or throat of a person who has had oral sex with an infected person.
Hepatitis symptoms
Hepatitis A, hepatitis B and hepatitis C are all contagious viral infections that affect your liver. Hepatitis B and C are the most serious of the three, but each can cause your liver to become inflamed.
Some people never develop signs or symptoms. But for those who do, signs and symptoms may occur several weeks after exposure and may include:
Fatigue
Nausea and vomiting
Abdominal pain or discomfort, especially in the area of your liver on your right side beneath your lower ribs
Loss of appetite
Fever
Dark urine
Muscle or joint pain
Itching
Yellowing of your skin and the whites of your eyes (jaundice)
Syphilis symptoms
Syphilis is a bacterial infection. The disease affects your genitals, skin and mucous membranes, but it can also involve many other parts of your body, including your brain and your heart.
The signs and symptoms of syphilis may occur in three stages — primary, secondary, and tertiary. Some people also experience latent syphilis, in which blood tests are positive for the bacteria but no symptoms are present.
At first, only a small, painless sore (chancre) may be present at the site of infection, usually the genitals, rectum, tongue or lips. As the disease worsens, symptoms may include:
Rash marked by red or reddish-brown, penny-sized sores over any area of your body, including your palms and soles
Fever
Enlarged lymph nodes
Fatigue and a vague feeling of discomfort
Soreness and aching
Without treatment, syphilis bacteria may spread, leading to serious internal organ damage and death years after the original infection.
Some of the signs and symptoms of late-stage syphilis include:
Lack of coordination
Numbness
Paralysis
Blindness
Dementia
There’s also a condition known as congenital syphilis, which occurs when a pregnant woman with syphilis passes the disease to her unborn infant. Congenital syphilis can be disabling, even life-threatening, so it’s important for pregnant women with syphilis to be treated.
Neurosyphilis
At any stage, syphilis can affect the nervous system. Neurosyphilis may cause no signs or symptoms, or it can cause:
Headache
Behavior changes
Movement problems
Prevention
Everyone should take certain preventive measures to avoid acquiring or transmitting STIs.
Get tested regularly
Typically, those with a vagina should get a Pap smear every 3 to 5 years. It’s also important to ask if you should be tested for any other STIs and whether the HPV vaccination is suggested.
According to the Office on Women’s Health, you should talk to your doctor about STI testing if you’re sexually active.
Use protection
Whether it’s for vaginal, anal, or oral sex, a condom or other barrier method can help protect both you and your partner. Female condoms and dental dams can provide a certain level of protection.
Spermicides, the birth control pill, and other forms of contraception may protect against pregnancy, but they don’t protect against STIs.
Communicate
Honest communication with both your doctor and your partner(s) about sexual history is essential.
STIs and pregnancy
A person can get STIs while pregnant. Because many conditions don’t show symptoms, some people don’t realize they’re living with one. For this reason, doctors may run a full STI panel at the beginning of a pregnancy.
These conditions can be life threatening to you and your baby. You can pass STIs on to your baby during pregnancy or birth, so early treatment is essential.
All bacterial STIs can be treated safely with antibiotics during pregnancy. Viral conditions can be treated with antivirals to prevent the likelihood of passing the condition to your child.
STIs and sexual assault
Some people will develop STIs as a direct result of a sexual assault. When women see a healthcare provider immediately following an assault, the healthcare provider tries to capture DNA and evaluate for injuries.
During this process, they check for potential STI diagnosis. If some time has passed since a sexual assault, you should still seek medical care. Your doctor or another healthcare provider can discuss possibly reporting the event, along with health-related concerns.
Depending on the person and their individual risk factors and medical history, the healthcare provider may prescribe preventive treatment, including:
Following up with a healthcare provider at the recommended time is important to ensure that the medications were effective and that no conditions need to be treated.
What to do once you’ve been diagnosed
Here are a few things you should do after being diagnosed with an STI:
Start any treatment your doctor prescribes for you immediately.
Contact your partner(s) and let them know that they need to get tested and treated, too.
Abstain from sex until the condition is either cured or until your doctor gives approval. In the case of bacterial conditions, you should wait until the medications have cured you and your partner.
For viral conditions, wait long enough for your partner to be on antiviral medications, if necessary, to reduce the risk of transmitting the condition to them. Your doctor will be able to give you the correct time frame.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
The main techniques for fetal assessment are the nonstress test, biophysical profile, modified biophysical profile, contraction stress test, and fetal movement count. Assessment of amniotic fluid volume (independent of the biophysical profile and modified biophysical profile) and Doppler velocimetry of fetal and funic vessels provide additional information about fetal status. Despite widespread use of these techniques, there is limited evidence to guide their optimal use or to demonstrate their effectiveness for improving perinatal outcomes.
Fetal surveillance is a broad term that refers to a variety of non-invasive tests that may be administered during a pregnancy in order to evaluate whether or not a baby is thriving in utero. These tests are typically ordered by obstetricians for women who are experiencing high risk pregnancies, and they are an additional means by which to manage and monitor both the mother’s and baby’s health and well-being.
What is Fetal Surveillance?
Fetal surveillance tests are a series of assessments that monitor a pregnancy when certain medical conditions are present or complications arise. Factors that can lead to a pregnancy being considered as high risk are diabetes, high blood pressure, multiple gestation (twins or more), post-term pregnancies (when gestation goes beyond 42 weeks), or women with pre-existing health conditions or previous high risk pregnancies.
However, if a physician orders fetal surveillance testing, it is not necessarily a cause for alarm. These tests should be regarded as an extra measure of vigilance for a mother and baby and are designed to ensure that the pregnancy and birth are as healthy and safe as possible.
What Are Fetal Surveillance Tests?
The types of tests a pregnant woman can receive as part of fetal surveillance will depend on each specific case. Assessments may include ultrasound, non-stress tests (NSTs), contraction stress tests (CST), and biophysical profiles (BPP).
Ultrasound
Ultrasounds performed in the case of fetal surveillance may be given periodically throughout a pregnancy and are often used to monitor the development of the fetus and the intrauterine conditions.
Non Stress Test (NST)
This test measures a baby’s heart rate and fetal movement over a specific period of time without any external factors being applied. For the NST, the fetal heart rate is monitored externally with a sensor that is attached to a belt and placed on the mother’s abdomen. This test poses no risk to the mother or child.
Contraction Stress Test (CST)
A Contraction Stress Test measures how a baby’s heart rate responds when the uterus contracts. As with the NTS, this test is administered with a belt sensor, but unlike the NST, contractions are physically or chemically induced and measures are taken under those altered conditions.
Biophysical Profiles (BPP)
The BPP uses a combination of ultrasound and NST to determine a baby’s fetal heart rate, breathing and body movements, fetal muscle tone, and the amount of amniotic fluid around the baby.
Who Should Receive Fetal Surveillance?
Fetal surveillance is typically only necessary in certain cases of high risk pregnancies. There is usually no need for such monitoring in low risk pregnancies and women should not feel the need to request these tests since fetal surveillance will only be administered if a doctor sees a need for them.
However, fetal surveillance may be required at any time during the pregnancy if complications should arise in an otherwise normal pregnancy. For instance, a decrease in a baby’s movements over a specific period of time may warrant a period of testing. Likewise, fetal surveillance may be curtailed if a baby is responding well, but if the baby does not respond to the monitoring as expected, additional recommendations will be made and measures taken.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Monitoring Mother and Baby’s Well-being
The doctors and staff at Kansas City ObGyn share the same goal with the new mothers we serve. It is our desire to see healthy pregnancies through to full term deliveries and fetal surveillance is sometimes a necessary step towards reaching that goal. We understand that it can be worrying to have a pregnancy categorized a “high risk” and to need special tests to ensure the pregnancy progressing as expected, but fetal surveillance should be cause for comfort since they allow our obstetricians to closely monitor and care for mother and child at any point throughout a pregnancy.
Techniques of Antepartum Fetal Surveillance
Several techniques for antepartum fetal surveillance currently in use are discussed in the ACOG bulletin. These include fetal movement assessment, nonstress test, contraction stress test, fetal biophysical profile, modified biophysical profile and umbilical artery Doppler velocimetry.
FETAL MOVEMENT ASSESSMENT
Fetal movement assessment occurs when the mother perceives a diminution in fetal movement. The mother counts fetal “kicks” as a means of antepartum fetal surveillance. The optimal number of movements and the ideal duration for counting movements have not been determined; however, numerous protocols have been reported and appear to be acceptable.
CONTRACTION STRESS TEST
The contraction stress test is based on the response of the fetal heart rate to uterine contractions. It is believed that fetal oxygenation will be transiently worsened by uterine contractions. In the fetus with suboptimal oxygenation, the resulting intermittent worsening in oxygenation will, in turn, lead to the fetal heart rate pattern of late decelerations. Uterine contractions also may provoke or accentuate a pattern of variable decelerations caused by fetal umbilical cord compression, which in some cases is associated with oligohydramnios.
The contraction stress test is interpreted by the presence or absence of late fetal heart rate decelerations, which are defined as decelerations that reach their nadir after the peak of the contraction and that usually persist beyond the end of the contraction. The results of the contraction stress test are categorized in the ACOG bulletin as follows:
Negative. No late or significant variable decelerations.
Positive. Late decelerations following 50 percent or more of contractions (even if the contraction frequency is fewer than three in 10 minutes).
Equivocal-suspicious. Intermittent late decelerations or significant variable decelerations.
Equivocal-hyperstimulatory. Fetal heart rate decelerations that occur in the presence of contractions that are more frequent than every two minutes or last longer than 90 seconds.
Unsatisfactory. Fewer than three contractions in 10 minutes or a tracing that is not interpretable.
Relative contraindications to the contraction stress test usually include conditions that are associated with an increased risk of preterm labor and delivery, uterine rupture or uterine bleeding. According to ACOG, these conditions include the following:
Preterm labor or certain patients at high risk of preterm labor.
Preterm membrane rupture.
History of extensive uterine surgery or classic cesarean delivery.
Known placenta previa.
NONSTRESS TEST
In the nonstress test, the heart rate of the fetus that is not acidotic or neurologically depressed will temporarily accelerate with fetal movement. Heart rate reactivity is believed to be a good indicator of normal fetal autonomic function. Loss of reactivity is commonly associated with a fetal sleep cycle but may result from any cause of central nervous system depression, including fetal acidosis.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Results of nonstress tests are classified as reactive or nonreactive. Various definitions of reactivity have been used. Most commonly, the nonstress test is considered reactive, or normal, if there are two or more fetal heart rate accelerations within a 20-minute period, with or without fetal movement discernible by the woman, according to ACOG. The nonreactive stress test lacks sufficient fetal heart rate accelerations over a 40-minute period. The nonstress test of the neurologically healthy preterm fetus is frequently nonreactive—from 24 to 28 weeks of gestation, up to 50 percent of nonstress tests may not be reactive, and from 28 to 32 weeks of gestation, 15 percent of nonstress tests are not reactive.
BIOPHYSICAL PROFILE
The biophysical profile discussed in the ACOG bulletin is a nonstress test plus four observations made by real-time ultrasonography. The five components of the biophysical profile are as follows: (1) nonstress test; (2) fetal breathing movements (one or more episodes of rhythmic fetal breathing movements of 30 seconds or more within 30 minutes); (3) fetal movement (three or more discrete body or limb movements within 30 minutes); (4) fetal tone (one or more episodes of extension of a fetal extremity with return to flexion, or opening or closing of a hand; and (5) determination of the amniotic fluid volume (a single vertical pocket of amniotic fluid exceeding 2 cm is considered evidence of adequate amniotic fluid).
Each of the components is given a score of 2 (normal or present as defined previously) or 0 (abnormal, absent or insufficient). A composite score of 8 or 10 is normal, a score of 6 is equivocal and a score of 4 or less is abnormal. In the presence of oligohydramnios, further evaluation is warranted regardless of the composite score.
MODIFIED BIOPHYSICAL PROFILE
During the late second or third trimester, amniotic fluid reflects fetal urine production. Placental dysfunction may cause diminished fetal renal perfusion, which can lead to oligohydramnios. Therefore, assessment of amniotic fluid volume can be used to evaluate long-term uteroplacental function. This led to the development of the modified biophysical profile.
The modified biophysical profile combines the non-stress test with the amniotic fluid index, which is the sum of measurements of the deepest cord-free amniotic fluid pocket in each of the abdominal quadrants, as an indicator of long-term function of the placenta. An amniotic fluid index of more than 5 cm is thought to be an adequate volume of amniotic fluid. The modified biophysical profile is considered normal if the nonstress test is reactive and the amniotic fluid index is greater than 5 cm and abnormal if the nonstress test is nonreactive or the amniotic fluid index is 5 cm or less.
UMBILICAL ARTERY DOPPLER VELOCIMETRY
Doppler ultrasonography is used to assess the hemodynamic components of vascular impedence. Umbilical artery Doppler flow velocimetry has been adapted as a fetal surveillance technique because it is believed that flow velocity waveforms in the umbilical artery of fetuses with normal growth differ from those of fetuses with growth restriction. The umbilical flow velocity waveform of a normally growing fetus has high-velocity diastolic flow, while in cases of intrauterine growth restriction, the umbilical artery diastolic flow is diminished. With extreme intrauterine growth restriction, the flow may be absent or even reversed. There is a high perinatal mortality rate among such pregnancies.
Indications for Antepartum Fetal Surveillance
The results of antepartum fetal surveillance have not definitively demonstrated improved perinatal outcome. Therefore, all indications for antepartum testing should be considered somewhat relative. Usually, antepartum fetal surveillance is used in pregnancies with a high risk of antepartum fetal death. Some of the conditions in which testing is appropriate include the following:
Maternal conditions: antiphospholipid syndrome, poorly controlled hyperthyroidism, hemoglobinopathies such as hemoglobin SS, SC or S-thalassemia, cyanotic heart disease, systemic lupus erythematosus, chronic renal disease, type 1 diabetes mellitus and hypertensive disorders.
Pregnancy-related conditions: pregnancy-induced hypertension, decreased fetal movement, oligohydramnios, polyhydramnios, intrauterine growth restriction, post-term pregnancy, moderate to severe isoimmunization, previous fetal demise (unexplained or recurrent risk) and multiple gestation with significant growth discrepancy.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Fetal Growth Restriction (FGR), formerly called Intrauterine Growth Restriction, refers to a condition in which an unborn baby is smaller than it should be because it is not growing at a normal rate inside the womb.
Delayed growth puts the baby at risk of certain health problems during pregnancy, delivery, and after birth. They include:
Low birth weight
Difficulty handling the stresses of vaginal delivery
Decreased oxygen levels
Hypoglycemia (low blood sugar)
Low resistance to infection
Low Apgar scores (a test given immediately after birth to evaluate the newborn’s physical condition and determine need for special medical care)
Meconium aspiration (inhalation of stools passed while in the uterus), which can lead to breathing problems
Trouble maintaining body temperature
Abnormally high red blood cell count
In the most severe cases, FGR can lead to stillbirth. It can also cause long-term growth problems
Intrauterine growth restriction (IUGR) is a common complication of pregnancy in developing countries, and carries an increased risk of perinatal mortality and morbidity. IUGR refers to a condition in which foetus (an unborn baby) is smaller or less developed than normal for the baby’s gender and gestational age. Gestational age is the age of a foetus or baby that starts on the first day of the mother’s last menstrual period.
In IUGR foetal weight is below the 10th percentile for gestational age as estimated by an ultrasound. At term, the birth weight less than 2,500 g (5lb, or 8oz) is considered as IUGR. Small for gestational age or fetal growth restriction are the other terms used for IUGR. The term intrauterine growth restriction has largely replaced the term intrauterine growth retardation.
IUGR is classified into two types-
Symmetric or primary IUGR: In this condition all internal organs are reduced in size. It is found in 20%-30% of all cases of IUGR.
Asymmetric or secondary IUGR: In this condition the head and brain are normal in size, but the abdomen is smaller. It is evident mostly in the 3rd trimester. It is more common and found in 70% to 80% of total IUGR cases.
Intrauterine growth restriction is observed in about 24% of newborns. In Asia IUGR accounts for nearly 75% of all affected infants. After prematurity IUGR is the second leading cause of perinatal morbidity and mortality.
Growth-restricted pregnancies are often complicated by a high rate of antepartum and intrapartum fetal distress and the need for cesarean delivery. These infants have many acute neonatal problems that include perinatal asphyxia, hypothermia (low body temperature), hypoglycemia (low blood sugar), and polycythemia (increased red blood cells), jaundice, feeding difficulties, feed intolerance, necrotizing enterocolitis, late-onset sepsis, and pulmonary hemorrhage.
When IUGR infants grow up long-term complications include growth retardation, neurodevelopment defects may occur. These infants are more likely to develop adult onset diseases because of fetal epigenetic changes.
Timely diagnosis (by assessment of fetal growth at each prenatal visit) and management of IUGR are the major activities in reducing perinatal morbidity and mortality.
Causes
IUGR has many causes related to mother, foetus and placenta (part that joins the mother and foetus). Various risk factors for IUGR can be summarized as-
A. Maternal causes –
Before pregnancy:
Low pre-pregnancy weight and small maternal size
Poor periconceptual nutritional status such as anemia, folate deficiency
Low socioeconomic status
Parity- none and more than 5 births
Recent pregnancy
During pregnancy:
Poor weight gain during pregnancy, especially in latter half
Moderate to heavy physical work
Chronic illness – such as malabsorption, diabetes, renal disease
Use of certain drugs, smoking, and alcohol
Pregnancy induced hypertension
Decreased oxygen availability such as in high altitude, severe maternal anemia
B. Uterine and placental factors:
Inadequate placental growth
Uterine malformations
Decreased utero-placental blood flow (such as in toxemias of pregnancy, diabetic vasculopathy)
Multiple gestations
C. Fetal causes include familial genetic and chromosomal abnormalities and intrauterine infections such as TORCH- which includes toxoplasmosis, other infections (syphilis, varicella-zoster, parvovirus B19), rubella, cytomegalovirus (CMV), and herpes infections.
Symmetric or primary IUGR is due to genetic or chromosomal causes, early gestational intrauterine infections (TORCH) and maternal alcohol use.
Asymmetric IUGR is more commonly due to extrinsic influences that affect the foetus later in gestation, such as preeclampsia, chronic hypertension, and uterine anomalies.
Symptoms
The main symptom of IUGR is a small for gestational age baby. During the antenatal checkup, a doctor measures the height of the uterus from the pubic bone to estimate the size of the fetus. After about the 20th week, uterine fundal height in centimeters is usually equal to the number of weeks of the pregnancy. A lag in fundal height of 4 cm or more with weeks of pregnancy suggests IUGR, and additional tests are required to confirm diagnosis.
During ultrasound, the baby’s estimated weight with IUGR is below the 10th percentile or less than that of 90% of babies of the same gestational age. At term, the birth weight less than 2,500 g (5 lb, 8 oz) is considered as IUGR. Not all babies that are born small have IUGR. In most severe cases IUGR can lead to stillbirth.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
At term birth, symptoms of IUGR are:
Baby is small all over or malnourished.
Thin, pale, loose and dry skin
Umbilical cord is thin and often stained with meconium
Diagnosis
One of the most important things when diagnosing IUGR is to know accurate gestational age of baby. Gestational age can be calculated by using the first day of last menstrual period (LMP) and also by early ultrasound calculations. Once the gestational age is known the following methods can be used to diagnose IUGR.
Fundal height: It is the simplest and most common method to diagnose IUGR. Fundal height is size of uterus measured as the distance from the pubic bone to the top of the uterus in centimeters. After the 20th week of pregnancy, the measure in centimeters usually corresponds with the number of weeks of pregnancy. A lag in fundal height of 4 cm or more suggests IUGR.
Weight checkups: Doctors routinely check and record the mother’s weight at every prenatal checkup. If a mother is not gaining weight properly, it could indicate a growth problem in her baby.
Ultrasound: It is used to measure the baby’s head and abdomen and compared with growth charts to estimate the baby’s weight. Ultrasound can also be used to determine amniotic fluid.
Doppler assessment: It is a technique that uses sound waves to measure the amount and speed of blood flow through the blood vessels. Doctors may use this test to check the flow of blood in the umbilical cord and vessels in the baby’s brain. Abnormal Doppler tests are diagnostic of IUGR
Complications
IUGR causes many health problems during pregnancy, delivery, and after birth. These include:
Difficulty during vaginal delivery
Low Apgar scores (a test done immediately after birth to evaluate the newborn’s physical condition to determine need for special medical care)
Meconium aspiration (inhalation of stools passed while in the uterus), which can lead to breathing problems
low birth weight
Hypoglycemia (low blood sugar)
High red blood cell count
Low resistance to infection
Difficulty in maintaining body temperature
Prevention
Although IUGR can occur even when a mother is perfectly healthy, still there are some measures to reduce the risk of IUGR and increase the chances of a healthy pregnancy and baby.
Care before pregnancy:
Providing care to women before and between pregnancies (inter-conception care) improves the chances of mothers and babies being healthy.
Advocating healthy eating and physical activity to women in their daily routine to improve weight and cardiovascular status before pregnancy.
Diagnosis and management of chronic diseases such as hypertension, diabetes before pregnancy.
Correction of anaemia/folic acid supplementation before pregnancy.
Care during pregnancy:
Pregnant mothers should take only those medicines which are prescribed by doctors.
Healthy diet should be advised to pregnant women with behavior change to encourage healthier eating patterns during pregnancy. Foods fortified with nutrients can be provided to pregnant women.
Pregnant women are advised to take enough rest with proper duration of sleep during night and an hour or two of rest in the afternoon.
Expectant mothers should follow healthy lifestyle habits. Tobacco use, smoking and alcohol intake should be avoided during pregnancy.
Care during delivery-
Delivery should be planned in health facilities having emergency obstetric care and neonatal care facilities.
Management
General management measures: These include treatment of maternal disease, good nutrition and advice for bed rest.
Preterm delivery is indicated if the fetus shows evidence of abnormal function on biophysical profile testing. Antenatal administration of steroids in preterm pregnancies and delivery at an institution with an emergency obstetric care and neonatal care unit is advised.
The foetus should be monitored continuously during labor to minimize fetal hypoxia.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
An antepartum haemorrhage (APH) is bleeding from the vagina that occurs after the 20th week of pregnancy and before the birth of your baby. The common causes of bleeding during pregnancy are cervical ectropion, vaginal infection, placental edge bleed, placenta praevia or placental abruption.
Cervical ectropion
The cells on the surface of the cervix often change in pregnancy and make the tissue more likely to bleed, particularly after sex. This is called cervical ectropion. This condition does not affect the pregnancy at all. If there is bleeding from the cervix it is important to ensure you are up to date with your PAP smear and it is normal.
Infection
Cervical and vaginal infections can also cause a small amount of vaginal bleeding (eg severe Thrush or Chlamydia) and you may be very uncomfortable. It is important to seek treatment from your doctor for these conditions.
Placental edge bleed
In the second half of your pregnancy, the lower-half of the uterus begins to stretch and grow. This can lead to the edge of the placenta separating from the wall of the uterus. In most cases bleeding will stop after a few hours, and your baby will not be adversely affected. However it is important that you contact the hospital immediately if you notice any bleeding.
Placenta praevia
Placenta praevia is diagnosed when the placenta grows in the lower part of the uterus and is located near to or actually covering the cervix. Placenta praevia is classified into four types:
Type I: the placenta is located in the lower part of the uterus but does not come close to the cervix. You can usually expect to birth vaginally with this type
Type II (or marginal) – the placenta touches but does not cover the cervix
Type III (or partial) – the placenta partially covers the cervix
Type IV (or complete) – the placenta completely covers the cervix
Types II, III and IV are associated with a risk of heavy bleeding in labour as the cervix dilates and, therefore caesarean birth is usually recommended.
Causes of placenta praevia
The cause of placenta praevia is often unknown but these are some of the factors that put women more at risk. :
previous caesarean birth or uterine surgery
previous placenta praevia
age above 35 years
multiple pregnancy twins or triplets etc.
multiple previous pregnancies
endometriosis
closely spaced pregnancies
placental abnormalities
abnormalities in the baby
smoking.
Diagnosis
As part of the 18–20 weeks ultrasound scan (USS) the site of the placenta is identified. Approximately one in five women will have a low-lying placenta at this time. A repeat USS will be recommended between 32 and 36 weeks of pregnancy depending on where the placenta is positioned at the earlier scan. By this time only 2 per cent of women will still have a low-lying placenta. Your doctor will discuss ongoing management and care. Most women with Type II, III & IV placenta praevia will need to give birth by caesarean section.
Placental abruption
Placental abruption occurs when part of the placenta separates from the wall of the uterus prior to term. A large amount of vaginal blood loss usually occurs. Some of the blood may however remain in the uterus and this can lead to a blood clot forming behind the placenta. The amount of vaginal blood loss seen is therefore, not an accurate measurement of the total amount of blood loss which has occurred.
If you have any blood loss or abdominal pain it is important to contact your midwife/obstetrician immediately. Some causes of vaginal bleeding are more serious than others so it is important to find out the reason as soon as possible.
Management
You may be admitted to hospital for observation and assessment of the cause of your bleeding. You will have an ultrasound scan and your baby may have a cardiotocograph (CTG) which checks your baby’s heart beat. Depending on how much bleeding has occurred, you may need to have an intravenous (IV) drip inserted and may require IV fluids. In severe circumstances you may require a blood transfusion or your baby may need to be born early. Initially you will be encouraged to rest in bed.
At this point in time, we recommend that you:
change sanitary pads at least every four hours while you have any blood loss (personal hygiene is very important to reduce the risk of infection)
do not use tampons
wipe from front to back after going to the toilet
do not go swimming
do not have baths or use a spa—please shower
do not have sexual intercourse
do not use any vaginal medications/creams.
If you experience an increase in vaginal bleeding, or abdominal pain or contractions it is important to notify the midwives or doctors as soon as it occurs.
If you have any bleeding in pregnancy there is an increased risk of your baby’s blood crossing into your blood stream. If you have a rhesus negative blood group you will be offered an injection of Anti-D immunoglobulin. THis should be discussed with your doctor.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Aetiology
No definite cause is diagnosed in about 50% of all women who present with APH; however, placenta praevia and placental abruption are the major identifiable causes:
Placenta praevia: insertion of the placenta, partially or fully, in the lower segment of the uterus. See the separate Placenta Praevia article.
Placental abruption: premature separation of a normally placed placenta. See the separate Placenta and Placental Problems article.
Local causes – eg, vulval or cervical infection, trauma or tumours.
Partner violence is common in pregnancy, occurring in 2.8% of pregnant women in a Canadian population-based study. It may result in APH. Women should be asked about this, particularly if there are repeated episodes. See the separate Domestic Violence article.
Vasa praevia: bleeding from fetal vessels in the fetal membranes, leading to high risk of fetal haemorrhage and death at rupture of the membranes. See the separate Placenta and Placental Problems article
Uterine rupture: rare but very dangerous for both mother and baby. See separate Uterine Rupture article
Inherited bleeding problems are very rare, occurring in 1 in 10,000 women[5].
Whilst risk factors for APH, in particular for placenta praevia and placental abruption, have been identified, APH cannot be predicted; 70% of cases of placental abruption occur in low-risk pregnancies.
There is limited evidence that APH can be prevented but women should be encouraged to change modifiable risk factors such as smoking and cocaine and amfetamine abuse.
Antenatal anaemia should be investigated and treated. Iron-deficiency anaemia not only reduces a woman’s tolerance to bleeding but may also contribute to uterine atony.
Presentation
Bleeding, which may be accompanied by pain (suggestive of abruption) or be painless (suggesting praevia).
Uterine contractions may be provoked.
There may be malpresentation or failure of the fetal head to engage, with placenta praevia.
There may be associated signs of fetal distress.
If the bleeding is severe, the mother may show signs of hypovolaemic shock; however, young, fit, pregnant women can compensate very well until sudden and catastrophic decompensation occurs.
Management
Always admit the patient to hospital for assessment and management, even if bleeding is only a very small amount; there may be a large amount of concealed bleeding with only a small amount of revealed vaginal bleeding. Phone 999/112/911 if there are any major concerns regarding maternal or fetal well-being.
Estimate amount of blood loss. This is often underestimated and needs to combined with an assessment of signs of clinical shock:
Minor haemorrhage = blood loss <50 ml and has stopped.
Major haemorrhage = blood loss 50-1000 ml with no signs of shock.
Massive haemorrhage = blood loss >1000 ml and/or signs of shock.
The mainstays of management of massive haemorrhage are effective communication between clinical staff, resuscitation, monitoring and accurate diagnosis of the underlying cause. The bleeding will be arrested by delivery of the fetus.
Severe bleeding: the mother’s life should take priority. Any decision regarding the delivery of the baby should wait until the mother’s condition is stable.
Fetal distress: urgent delivery of the baby, irrespective of gestational age. Fetal compromise is an important indicator of reduced circulating blood volume.
No vaginal examination should be attempted, at least until a placenta praevia is excluded by ultrasound. It may initiate torrential bleeding from a placenta praevia.
Resuscitation can be inadequate because of underestimation of blood loss and misleading maternal response, especially in small women. For example, a woman who weighs 55 kg will have lost almost 30% of her blood volume if she loses 1500 ml of blood, whereas for a woman of 70 kg, this represents about 20% of her blood volume[2].
Blood tests:
FBC and ‘group and save’. NB: initial Hb may not reflect degree of blood loss. Low platelet count may suggest significant abruption.
Clotting studies, if platelet count is abnormal, as coagulopathy is common and should be anticipated.
Crossmatch four units and check U&Es and LFTs, if there is major or massive haemorrhage.
Gentle palpation of the abdomen to determine the gestational age of the fetus, presentation and position.
Fetal monitoring.
Arrange urgent ultrasound to exclude placenta praevia; ultrasound cannot exclude placental abruption, which is a clinical diagnosis.
With every episode of bleeding, a rhesus-negative woman should have a Kleihauer test and be given prophylactic anti-D immunoglobulin.
Maternal corticosteroids should be offered to any woman at risk of preterm birth, who is between 24+0 and 35+6 weeks of gestation.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Further management
Further management will depend on fetal distress, the cause of the APH, the extent of bleeding and gestation.
All women need to be assessed individually, taking into account not only the amount of blood loss but also any relevant current or past medical and obstetric history.
Placenta praevia: see the separate Placenta Praevia article.
Moderate or severe placental abruption: see the separate Placenta and Placental Problems article.
Complications
Premature labour.
Disseminated intravascular coagulopathy.
Acute kidney injury.
Postpartum haemorrhage.
Placenta accreta: this may complicate cases of placenta praevia but is rare in the absence of placenta praevia or previous caesarean section. See the separate Placenta and Placental Problems article.
Anaemia.
Infection.
Prolonged hospital stay.
Psychological sequelae.
Fetal complications:
Fetal hypoxia.
Fetal growth restriction.
Prematurity, both iatrogenic and spontaneous.
Fetal death.
Prognosis
One population-based study found that bleeding in the second half of pregnancy is an independent risk factor for perinatal mortality.
Maternal mortality is low if managed by an experienced obstetrician and if no vaginal examination is performed before admission to hospital.
Perinatal mortality is 119 per 1,000 births complicated by abruption.
In pregnancies when the cause of APH is not known, there is still a greater risk of preterm delivery and induced labour but no increase in perinatal mortality after adjusting for gestational age
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Pregnancy stresses your heart and circulatory system. During pregnancy, your blood volume increases by 30 to 50 percent to nourish your growing baby, your heart pumps more blood each minute and your heart rate increases.
Labor and delivery add to your heart’s workload, too. During labor — particularly when you push — you’ll have abrupt changes in blood flow and pressure. It takes several weeks after delivery for the stresses on the heart to return to the levels they were before you became pregnant.
Heart disorders account for about 10% of maternal obstetric deaths. In the US, because incidence of rheumatic heart disease has markedly declined, most heart problems during pregnancy result from congenital heart disease. However, in Southeast Asia, Africa, India, the Middle East, and parts of Australia and New Zealand, rheumatic heart disease is still common.
Despite dramatic improvements in survival and quality of life for patients with severe congenital heart defects and other heart disorders, pregnancy remains inadvisable for women with certain high-risk disorders such as the following:
Pulmonary hypertension (pulmonary artery systolic pressure > 25 mm Hg) caused by any condition, including Eisenmenger syndrome
Coarctation of the aorta if uncorrected or if accompanied by an aneurysm
Marfan syndrome with aortic root diameter of > 4.5 cm
Severe symptomatic aortic stenosis or severe mitral stenosis
Bicuspid aortic valve with ascending aorta diameter > 50 mm
A single ventricle and impaired systolic function (whether treated with the Fontan procedure or not)
Cardiomyopathy with ejection fraction < 30% or New York Heart Association (NYHA) class III or IV heart failure
What are the risks?
The risks depend on the nature and severity of your heart condition. For example:
Heart rhythm issues. Minor abnormalities in heart rhythm are common during pregnancy. They’re not usually cause for concern. If you need treatment for an arrhythmia, you’ll likely be given medication, the same as you would if you weren’t pregnant.
Heart valve issues. Having an artificial heart valve or scarring or malformation of your heart or valves can increase your risk of complications during pregnancy. If your valves aren’t working properly, you might have trouble tolerating the increased blood flow that occurs during pregnancy. In addition, artificial or abnormal valves carry an increased risk of a potentially life-threatening infection of the lining of the heart (endocarditis) and heart valves. Mechanical artificial heart valves also pose serious risks during pregnancy due to the need to adjust use of blood thinners, the potential for life-threatening clotting (thrombosis) of heart valves. Taking blood thinners can also put your developing baby at risk.
Congestive heart failure. As blood volume increases, congestive heart failure can worsen.
Congenital heart defect If you were born with a heart problem, your baby has a greater risk of developing some type of heart defect, too. You might also be at risk for heart problems occurring during pregnancy and of premature birth.
Pre-existing cardiovascular conditions and pregnancy
Congenital heart conditions and pregnancy
Congenital heart defects are the most common heart problems that affect women of childbearing age. These include shunt lesions, obstructive lesions, complex lesions and cyanotic heart disease.
Shunt lesions
Shunt lesions are the simplest and most common congenital heart defects. Shunts include atrial septal defect (ASD), which is a hole between the upper chambers of the heart; ventricular septal defect (VSD), which is a hole between the lower chambers of the heart; and patent ductus arteriosus (PDA), which means there is abnormal blood flow between the aorta and pulmonary artery. If the hole is large, a fair amount of blood from the left side of the heart will flow back into the right side of the heart. The blood gets pumped back to the lungs again and causes strain on the heart. This can lead to an enlarged heart, abnormal heart rhythms and increased pressure in the lungs (pulmonary hypertension). Pulmonary hypertension, when severe, can cause the blood flow across the shunt to move in reverse. This can cause low levels of oxygen in the blood (cyanosis). In such cases, pregnancy is not recommended due to the high risk of the mother dying.
Obstructive Lesions
Obstructive lesions reduce the amount of blood flow to the heart and the body’s major blood vessels. One such lesion, aortic coarctation is a narrowing in the descending aorta, which is the largest artery in the body. Aortic coarctation can cause a pregnant woman to have high blood pressure. The condition can also keep the placenta (the collection of blood vessels that supplies the baby with blood) from getting enough blood. Depending on how severe the narrowing is, you may need a procedure before or during pregnancy to keep you and the baby safe during pregnancy.
Complex lesions
Complex lesions include transposition of the great arteries. This means the aorta and pulmonary arteries are attached to the wrong ventricles (bottom chambers of the heart). Surgery to repair the problem can cause problems with the heart chambers, especially if the right ventricle pumps blood out to the body (this is usually the job of the left ventricle). In this case, the problem can cause heart failure and leaky heart valves, and the conditions can become worse during pregnancy. If you have this condition, you will need to be closely followed during pregnancy.
Cyanotic heart disease includes tetralogy of Fallot. This is a condition that includes a VSD, narrowing of the pulmonary valve and abnormal configuration of the aorta. Treatment usually keeps cyanosis from recurring. However, the repair can cause a leaky pulmonary valve, and that problem can lead to heart failure and heart rhythm disturbances. If you have a leaky pulmonary valve, you may need to have it corrected before you become pregnant.
In general, most women with congenital heart defects, especially those who have had corrective surgeries, can safely become pregnant. However, the outcome of the pregnancy and risk of complications depends on the type of heart defect you have, how severe your symptoms are, and whether you have heart muscle dysfunction, heart rhythm disturbances or pulmonary hypertension with related lung disease. Your pregnancy can also be affected if you have had particular types of heart surgery.
Valve disease and pregnancy
Aortic valve stenosis means the aortic valve (the valve between the left ventricle and the aorta) is narrowed or stiff. If the narrowing is severe, the heart has to work harder to pump the increased blood volume out of the narrowed valve. This, in turn, can cause the left ventricle (the major pumping chamber of the heart to enlarge – a condition called hypertrophy). Over time, symptoms of heart failure can occur or become worse and increase the risk of long-term complications for the mother.
One common cause of aortic valve stenosis is bicuspid aortic valve disease. This is a congenital heart condition in which there are only two leaflets (also called cusps), instead of the normal three leaflets inside the valve. The leaflets open and close to keep blood flowing in the right direction and prevent backflow. Without the third leaflet, the valve can become narrowed or stiff.
Women with bicuspid aortic valve disease or any type of aortic valve stenosis need to be evaluated by a cardiologist before planning a pregnancy. In some cases, surgery is recommended to correct the valve before pregnancy.
Mitral valve stenosis means the mitral valve (the valve between the left atrium and left ventricle) is narrowed. This condition is often caused by rheumatic fever.
The increased blood volume and increased heart rate that occur during pregnancy can make symptoms of mitral stenosis get worse. The left atrium can become bigger and cause a rapid, irregular heart rhythm called atrial fibrillation. In addition, the problem can cause heart failure symptoms (shortness of breath, irregular heart beat, fatigue and swelling/edema). This can increase the risk to the mother. If you have mitral valve stenosis, you may need to take medications while you are pregnant. Your doctor may also recommend an catheter-based procedure, called percutaneous valvuloplasty, to correct the narrowed valve while you are pregnant. It is important to have mitral stenosis evaluated before you become pregnant. In some cases, surgery or valvuloplasty to correct the valve will be recommended before pregnancy.
Mitral valve prolapse is a common condition that usually doesn’t cause symptoms or require treatment. Most patients with mitral valve prolapse tolerate pregnancy well. If the prolapse causes a severe leak, you may need treatment before you become pregnant. Be sure to talk to your doctor if you plan to become pregnant and follow any recommendations.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Pregnancy in women with prosthetic (artificial) valves
Women who have artificial heart valves may experience complications during pregnancy because:
Women who have an artificial heart valve need to take lifelong anticoagulant medication, and certain anticoagulant medications can be harmful to the baby. There is controversy about which anticoagulant medication regimen is best during pregnancy.*
During pregnancy, there is an increased risk of blood clots.
*Use of warfarin, heparin, aspirin, and combinations of these anticoagulant medications have been suggested and compared. The most recent recommendations from the European Heart Association are to use heparin during the first trimester, followed by warfarin up to the 36th week of pregnancy, and subsequent replacement with heparin until delivery OR to use oral anticoagulation medication throughout pregnancy, until the 36th week, followed by heparin until delivery.
The use of warfarin is less harmful if the dose is kept to less than 5 mg. In addition, other specialists have recommended the addition of low-dose aspirin to treat women who are at high risk.
If you have a prosthetic valve and are taking an anticoagulant medication, it is very important to be evaluated by a cardiologist before planning a pregnancy. The cardiologist will talk to you about your potential risks and determine the best anticoagulant therapy routine for you.
In addition, ask your doctor what precautions you should continue to follow to prevent endocarditis.
Aorta Disease and pregnancy
Women who have conditions that affect the aorta, such as aortic aneurysm, dilated aorta, or connective tissue disorders such as Marfan syndrome, are at increased risk during pregnancy.
Pressure in the aorta increases during pregnancy and when bearing down during labor and delivery. This extra pressure increases the risk of an aortic dissection or rupture, which can be life-threatening.
It is very important for women who have aorta disease to be evaluated by a cardiologist before planning a pregnancy. A thorough evaluation of your condition will provide the physician with information about the potential risks of pregnancy. It is also important to note that some conditions, such as Marfan syndrome, are genetic and can be passed down to children, so genetic counseling may be recommended.
Cardiovascular disorders that may develop during pregnancy
Peripartum cardiomyopathy
Peripartum cardiomyopathy is a rare condition. It is when heart failure develops in the last month of pregnancy or within five months after delivery. The cause of peripartum cardiomyopathy remains unknown. Certain patients, including those with multiple pregnancies and those of African descent, are at greatest risk. Women with peripartum cardiomyopathy have symptoms of heart failure. After pregnancy, the heart usually returns to its normal size and function. But, some women continue to have poor left ventricular function and symptoms. Women with peripartum cardiomyopathy have an increased risk of complications during future pregnancies, especially if the heart dysfunction continues.
Hypertension (high blood pressure)
About 6% to 8% of women develop high blood pressure, also called hypertension, during pregnancy. This is called pregnancy-induced hypertension (PIH) and is related to preeclampsia, toxemia, or toxemia of pregnancy. Symptoms of PIH include high blood pressure, swelling due to fluid retention, and protein in the urine. Pregnancy-induced hypertension can be harmful to the mother and the baby. To learn more about who is at risk for PIH, symptoms of PIH, and how PIH is diagnosed and treated, click on the following links:
Cleveland Clinic – Pregnancy-Induced Hypertension
Cleveland Clinic – Preeclampsia and Eclampsia
American Heart Association – Pregnancy and High Blood Pressure
Myocardial infarction
Heart attack (myocardial infarction) is fortunately a very rare but potentially deadly complication that can occur during pregnancy or during the first few weeks afterwards. A heart attack can be caused by many things. Patients with coronary artery disease (“hardening of the arteries”) can have a myocardial infarction if the plaque inside their arteries ruptures. This problem is becoming more common, since many women wait until later in life to become pregnant. Other causes of a heart attack include a spontaneous blood clot inside a coronary vessel (because pregnancy increases the risk of blood clots) and coronary dissection (a weakening of the vessel wall that leads to a spontaneous tear and clotting). If you have a heart attack, it is critical to get emergency help. Treatment will be focused on ensuring your survival.
Heart Murmur
Sometimes, the increase in blood volume during pregnancy can cause a heart murmur(an abnormal “swishing” sound). In most cases, the murmur is harmless. But in rare cases, it could mean there’s a problem with a heart valve. Your doctor can evaluate your condition and determine the cause of the murmur.
Arrhythmias and pregnancy
Abnormal heartbeats (arrhythmias) during pregnancy are common. Women who have never had an arrhythmia or heart problem may first develop an arrhythmia during pregnancy. When an arrhythmia develops during pregnancy, it can be a sign of a heart condition you didn’t know you had. Most of the time, the arrhythmia causes little in the way of symptoms and does not require treatment. If you have symptoms, your doctor may order tests to determine the type arrhythmia you have and attempt to determine its cause.
Special considerations before and during pregnancy
Congenital heart defects (in either the mother or father) increase the baby’s risk of having a heart problem. Your cardiologist may refer you to a geneticist for further evaluation. A fetal echocardiogram may be recommended to check the baby’s heart for possible defects. This test is usually done in the 18th week of pregnancy.
If you have been diagnosed with a congenital heart defect, a cardiologist should evaluate your heart condition before you plan a pregnancy. The cardiologist will talk to you about the possible risks of pregnancy and can work with your healthcare team to monitor your health and your baby’s health while you are pregnant.
How can I prevent complications?
Taking good care of yourself is the best way to take care of your baby. For example:
Keep your prenatal appointments. Visit your health care provider regularly throughout your pregnancy.
Take your medication as prescribed. Your health care provider will prescribe the safest medication at the most appropriate dose.
Get plenty of rest. Take a daily nap, if you can, and avoid strenuous physical activities.
Monitor your weight gain. Gaining the right amount of weight supports your baby’s growth and development. Gaining too much weight places additional stress on your heart.
Manage anxiety. Ask questions about your progress. Find out what to expect during labor and delivery. Knowing what’s happening can help you feel more at ease.
Know what’s off-limits. Avoid smoking, alcohol, caffeine and illegal drugs.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
When you’re pregnant, you may develop anemia. When you have anemia, your blood doesn’t have enough healthy red blood cells to carry oxygen to your tissues and to your baby.
During pregnancy, your body produces more blood to support the growth of your baby. If you’re not getting enough iron or certain other nutrients, your body might not be able to produce the amount of red blood cells it needs to make this additional blood.
It’s normal to have mild anemia when you are pregnant. But you may have more severe anemia from low iron or vitamin levels or from other reasons.
Anemia can leave you feeling tired and weak. If it is severe but goes untreated, it can increase your risk of serious complications like preterm delivery.
Normally during pregnancy, erythroid hyperplasia of the marrow occurs, and red blood cell (RBC) mass increases. However, a disproportionate increase in plasma volume results in hemodilution (hydremia of pregnancy): hematocrit (Hct) decreases from between 38% and 45% in healthy women who are not pregnant to about 34% during late single pregnancy and to 30% during late multifetal pregnancy. Thus during pregnancy, anemia is defined as hemoglobin (Hb) < 10 g/dL (Hct < 30%). If Hb is < 11.5 g/dL at the onset of pregnancy, women may be treated prophylactically because subsequent hemodilution usually reduces Hb to < 10 g/dL. Despite hemodilution, oxygen-carrying capacity remains normal throughout pregnancy. Hct normally increases immediately after birth.
Anemia occurs in up to one third of women during the 3rd trimester. The most common causes are
Iron deficiency
Folate deficiency
Obstetricians, in consultation with a perinatologist, should evaluate anemia in pregnant Jehovah’s Witness patients (who are likely to refuse blood transfusions) as soon as possible.
Types of Anemia During Pregnancy
Several types of anemia can develop during pregnancy. These include:
Iron-deficiency anemia
Folate-deficiency anemia
Vitamin B12 deficiency
Here’s why these types of anemia may develop:
Iron-deficiency anemia. This type of anemia occurs when the body doesn’t have enough iron to produce adequate amounts of hemoglobin. That’s a protein in red blood cells. It carries oxygen from the lungs to the rest of the body.
In iron-deficiency anemia, the blood cannot carry enough oxygen to tissues throughout the body.
Iron deficiency is the most common cause of anemia in pregnancy.
Folate-deficiency anemia. Folate is the vitamin found naturally in certain foods like green leafy vegetables A type of B vitamin, the body needs folate to produce new cells, including healthy red blood cells.
During pregnancy, women need extra folate. But sometimes they don’t get enough from their diet. When that happens, the body can’t make enough normal red blood cells to transport oxygen to tissues throughout the body. Man made supplements of folate are called folic acid.
Folate deficiency can directly contribute to certain types of birth defects, such as neural tube abnormalities (spina bifida) and low birth weight.
Vitamin B12 deficiency. The body needs vitamin B12 to form healthy red blood cells. When a pregnant woman doesn’t get enough vitamin B12 from their diet, their body can’t produce enough healthy red blood cells. Women who don’t eat meat, poultry, dairy products, and eggs have a greater risk of developing vitamin B12 deficiency, which may contribute to birth defects, such as neural tube abnormalities, and could lead to preterm labor.
Blood loss during and after delivery can also cause anemia.
Symptoms and Signs
Early symptoms of anemia are usually nonexistent or nonspecific (eg, fatigue, weakness, light-headedness, mild dyspnea during exertion). Other symptoms and signs may include pallor and, if anemia is severe, tachycardia or hypotension.
Anemia increases risk of
Preterm delivery
Postpartum maternal infections
Diagnosis
Complete blood count (CBC), followed by testing based on mean corpuscular value (MCV) value
Diagnosis of anemia begins with CBC; usually, if women have anemia, subsequent testing is based on whether the MCV is low (< 79 fL) or high (> 100 fL): Lab Test Ferritin
For microcytic anemias: Evaluation includes testing for iron deficiency (measuring serum ferritin) and hemoglobinopathies (using hemoglobin electrophoresis). If these tests are nondiagnostic and there is no response to empiric treatment, consultation with a hematologist is usually warranted.
For macrocytic anemias: Evaluation includes serum folate and vitamin B12 levels.
For anemia with mixed causes: Evaluation for both types is required.
Risk Factors for Anemia in Pregnancy
All pregnant women are at risk for becoming anemic. That’s because they need more iron and folic acid than usual. But the risk is higher if you:
Are pregnant with multiples (more than one child)
Have had two pregnancies close together
Vomit a lot because of morning sickness
Are a pregnant teenager
Don’t eat enough foods that are rich in iron
Had anemia before you became pregnant
Symptoms of Anemia During Pregnancy
The most common symptoms of anemia during pregnancy are:
Pale skin, lips, and nails
Feeling tired or weak
Dizziness
Shortness of breath
Rapid heartbeat
Trouble concentrating
In the early stages of anemia, you may not have obvious symptoms. And many of the symptoms are ones that you might have while pregnant even if you’re not anemic. So be sure to get routine blood tests to check for anemia at your prenatal appointments.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Risks of Anemia in Pregnancy
Severe or untreated iron-deficiency anemia during pregnancy can increase your risk of having:
A preterm or low-birth-weight baby
A blood transfusion (if you lose a significant amount of blood during delivery)
Postpartum depression
A baby with anemia
A child with developmental delays
Untreated folate deficiency can increase your risk of having a:
Preterm or low-birth-weight baby
Baby with a serious birth defect of the spine or brain (neural tube defects)
Untreated vitamin B12 deficiency can also raise your risk of having a baby with neural tube defects.
Tests for Anemia
During your first prenatal appointment, you’ll get a blood test so your doctor can check whether you have anemia. Blood tests typically include;
Hemoglobin test. It measures the amount of hemoglobin — an iron-rich protein in red blood cells that carries oxygen from the lungs to tissues in the body.
Hematocrit test. It measures the percentage of red blood cells in a sample of blood.
If you have lower than normal levels of hemoglobin or hematocrit, you may have iron-deficiency anemia. Your doctor may check other blood tests to determine if you have iron deficiency or another cause for your anemia.
Even if you don’t have anemia at the beginning of your pregnancy, your doctor will most likely recommend that you get another blood test to check for anemia in your second or third trimester.
Treatment for Anemia
If you are anemic during your pregnancy, you may need to start taking an iron supplement and/or folic acid supplement in addition to your prenatal vitamins. Your doctor may also suggest that you add more foods that are high in iron and folic acid to your diet.
In addition, you’ll be asked to return for another blood test after a specific period of time so your doctor can check that your hemoglobin and hematocrit levels are improving.
To treat vitamin B12 deficiency, your doctor may recommend that you take a vitamin B12 supplement.
The doctor may also recommend that you include more animal foods in your diet, such as:
meat
eggs
dairy products
Your OB may refer you to a hematologist, a doctor who specializes in anemia/ blood issues. The specialist may see you throughout the pregnancy and help your OB manage the anemia.
Preventing Anemia
To prevent anemia during pregnancy, make sure you get enough iron. Eat well-balanced meals and add more foods that are high in iron to your diet.
Aim for at least three servings a day of iron-rich foods, such as:
lean red meat, poultry, and fish
leafy, dark green vegetables (such as spinach, broccoli, and kale)
iron-enriched cereals and grains
beans, lentils, and tofu
nuts and seeds
eggs
Foods that are high in vitamin C can help your body absorb more iron. These include:
citrus fruits and juices
strawberries
kiwis
tomatoes
bell peppers
Try eating those foods at the same time that you eat iron-rich foods. For example, you could drink a glass of orange juice and eat an iron-fortified cereal for breakfast.
Also, choose foods that are high in folate to help prevent folate deficiency. These include:
leafy green vegetables
citrus fruits and juices
dried beans
breads and cereals fortified with folic acid
Follow your doctor’s instructions for taking a prenatal vitamin that contains a sufficient amount of iron and folic acid.
Vegetarians and vegans should talk with their doctor about whether they should take a vitamin B12 supplement when they’re pregnant and breastfeeding.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Iron Deficiency Anemia in Pregnancy
About 95% of anemia cases during pregnancy are iron deficiency anemia. The cause is usually
Inadequate dietary intake (especially in adolescent girls)
A previous pregnancy
The normal recurrent loss of iron in menstrual blood (which approximates the amount normally ingested each month and thus prevents iron stores from building up) before the woman became pregnant
Diagnosis
Measurement of serum iron, ferritin, and transferrin
Typically, Hct is ≤ 30%, and MCV is < 79 fL. Decreased serum iron and ferritin and increased serum transferrin levels confirm the diagnosis of iron deficiency anemia.
Treatment
Usually ferrous sulfate 325 mg po once/day
One 325-mg ferrous sulfate tablet taken midmorning is usually effective. Higher or more frequent doses increase GI adverse effects, especially constipation, and one dose blocks absorption of the next dose, thereby reducing percentage intake.
About 20% of pregnant women do not absorb enough supplemental oral iron; a few of them require parenteral therapy, usually iron dextran 100 mg IM every other day for a total of ≥ 1000 mg over 3 weeks. Hct or Hb is measured weekly to determine response. If iron supplements are ineffective, concomitant folate deficiency should be suspected.
Neonates of mothers with iron deficiency anemia usually have a normal Hct but decreased total iron stores and a need for early dietary iron supplements.
Prevention
Although the practice is controversial, iron supplements (usually ferrous sulfate 325 mg po once/day) are usually given routinely to pregnant women to prevent depletion of body iron stores and prevent the anemia that may result from abnormal bleeding or a subsequent pregnancy.
Folate Deficiency Anemia in Pregnancy
Folate deficiency increases risk of neural tube defects and possibly fetal alcohol syndrome. Deficiency occurs in 0.5 to 1.5% of pregnant women; megaloblastic macrocytic anemia is present if deficiency is moderate or severe.
Rarely, severe anemia and glossitis occur.
Diagnosis
Measurement of serum folate
Folate deficiency is suspected if CBC shows anemia with macrocytic indices or high RBC distribution width (RDW). Low serum folate levels confirm the diagnosis.
Treatment
Folic acid 1 mg po bid
Treatment is folic acid 1 mg po bid.
Severe megaloblastic anemia may warrant bone marrow examination and further treatment in a hospital.
Prevention
For prevention, all pregnant women and women who are trying to conceive are given folic acid 0.4 to 0.8 mg po once/day. Women who have had a fetus with spina bifida should take 4 mg once/day, starting before conception.
Hemoglobinopathies in Pregnancy
During pregnancy, hemoglobinopathies, particularly sickle cell disease, Hb S-C disease, and beta- and alpha-thalassemia, can worsen maternal and perinatal outcomes. Genetic screening genetic screening for some of these disorders is available.
Preexisting sickle cell disease, particularly if severe, increases risk of the following:
Anemia almost always becomes more severe as pregnancy progresses. Sickle cell trait increases the risk of UTIs but is not associated with severe pregnancy-related complications.
Treatment of sickle cell disease during pregnancy is complex. Painful crises should be treated aggressively. Prophylactic exchange transfusions to keep Hb A at ≥ 60% reduce risk of hemolytic crises and pulmonary complications, but they are not routinely recommended because they increase risk of transfusion reactions, hepatitis, HIV transmission, and blood group isoimmunization. Prophylactic transfusion does not appear to decrease perinatal risk. Therapeutic transfusion is indicated for the following:
Symptomatic anemia
Heart failure
Severe bacterial infection
Severe complications of labor and delivery (eg, bleeding, sepsis)
Hb S-C disease may first cause symptoms during pregnancy. The disease increases risk of pulmonary infarction by occasionally causing bony spicule embolization. Effects on the fetus are uncommon but, if they occur, often include fetal growth restriction.
Sickle cell–beta-thalassemia is similar to Hb S-C disease but is less common and more benign.
Alpha-thalassemia does not cause maternal morbidity, but if the fetus is homozygous, hydrops and fetal death occur during the 2nd or early 3rd trimester.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Women who develop hypertension after 20 weeks’ gestation and who do not have proteinuria or other criteria for preeclampsia are diagnosed with gestational hypertension. This is a provisional diagnosis that includes women who eventually develop preeclampsia, those with unrecognized chronic hypertension (diagnosed by persistently elevated BP beyond 12 weeks postpartum), and women with transient hypertension of pregnancy. Approximately 50% of women diagnosed with gestational hypertension between 24 and 35 weeks’ gestation ultimately develop preeclampsia. Management of gestational hypertension is similar to that of preeclampsia, with expectant monitoring and labor induction at 37 weeks’ gestation
Worldwide there is disagreement about many aspects of the classification, diagnosis, and management of the hypertensive disorders of pregnancy. This lack of consensus hampers our ability to study not only the immediate rates of adverse maternal and fetal outcomes for the various hypertensive disorders in pregnancy, particularly preeclampsia, but also the long-term health outcomes of women and babies who survive this condition. It also impacts on research into the pathophysiology of this condition and has almost certainly delayed the development of effective screening tests and treatments, leading to poorer pregnancy outcomes.
One scholarly review of available guidelines has shown broad agreement in the following areas:
Definitions of hypertension, proteinuria, chronic hypertension, and gestational hypertension;
Prevention of preeclampsia with low-dose aspirin and supplemental calcium (if low calcium intake);
Treatment of severe hypertension;
Use of MgSO4 for eclampsia and severe preeclampsia;
Use of antenatal corticosteroids to enhance fetal lung maturity at <34 weeks’ gestation if delivery is likely within the next 7 days;
Delivery for preeclampsia at term; and
Oxytocin in the third stage of labor.
However, in this analysis, there was little or no agreement on
The definition of preeclampsia;
Target BP when hypertension is not severe;
Timing of delivery for women with chronic hypertension, gestational hypertension, or preterm preeclampsia;
Use of MgSO4 for preeclampsia that is not severe; and
Postpartum maternal monitoring.
Classification
1.Hypertension in pregnancy may be chronic (predat-ing pregnancy or diagnosed before 20 weeks of preg-nancy) or de novo (either preeclampsia or gestational hypertension).
2.Chronic hypertension is associated with adverse mater-nal and fetal outcomes and is best managed by tightly controlling maternal blood pressure (BP, 110–140/85 mmHg), monitoring fetal growth, and repeatedly as-sessing for the development of preeclampsia and ma-ternal complications. This can be done in an outpatient setting.
3.White-coat hypertension refers to elevated office/clin-ic (≥140/90 mmHg) BP, but normal BP measured at home or work (<135/85 mmHg); it is not an entirely benign condition and conveys an increased risk for preeclampsia.
4.Masked hypertension is another form of hypertension, more difficult to diagnose, characterized by BP that is normal at a clinic or office visit but elevated at other times, most typically diagnosed by 24-hour ambula-tory BP monitoring (ABPM) or automated home BP monitoring.
5.Gestational hypertension is hypertension arising de novo after 20 weeks’ gestation in the absence of protein-uria and without biochemical or hematological abnor-malities. It is usually not accompanied by fetal growth restriction. Outcomes in pregnancies complicated by gestational hypertension are normally good, but about a quarter of women with gestational hypertension (par-ticularly those who present at <34 weeks) will progress to preeclampsia and have poorer outcomes.
6.Preeclampsia is a complex medical disorder; worldwide, each year, it is responsible for >500000 fetal and neo-natal deaths and >70000 maternal deaths. Preeclampsia can deteriorate rapidly and without warning; we do not recommend classifying it as mild or severe
7. Proteinuria is not mandatory for a diagnosis of pre-eclampsia. Rather, this is diagnosed by the presence of de novo hypertension after 20 weeks’ gestation accom-panied by proteinuria and/or evidence of maternal acute kidney injury (AKI), liver dysfunction, neurological fea-tures, hemolysis or thrombocytopenia, or fetal growth restriction. Preeclampsia may develop or be recognized for the first time intrapartum or early postpartum in some cases.
8.The hemolysis, elevated liver enzymes, low platelets syndrome is a (serious) manifestation of preeclampsia and not a separate disorder.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Diagnosis of Hypertension and Proteinuria
1.Home BP monitoring is a useful adjunct in the manage-ment of chronic hypertension and is mandatory in the management of white-coat hypertension.
2.Proteinuria is optimally assessed by screening with au-tomated dipstick urinalysis and then if positive quantify-ing with a urine protein/creatinine ratio. A ratio ≥30 mg/mmol (0.3 mg/mg) is abnormal.
Pathophysiology of Preeclampsia
Abnormal placental implantation (defects in trophoblasts and spiral arterioles)
Angiogenic factors (low level of placental growth factor)
Preeclampsia in a previous pregnancy (particularly if severe or before 32 weeks’ gestation)
7
Diabetes mellitus (preexisting)
3
Family history of preeclampsia (first-generation relative)
3
Multiple gestation
3
Nulliparity
3
Elevated body mass index
2
Maternal age > 40 years
1.6
Chronic hypertension or renal disease
Management
Regardless of the hypertensive disorder of pregnancy, BP requires urgent treatment in a monitored setting when severe (>160/110 mm Hg); acceptable agents for this include oral nifedipine or intravenous labetalol or hydralazine. Oral labetalol may be used if these treatments are unavailable.
Regardless of the hypertensive disorder of pregnancy, BPs consistently at or >140/90 mm Hg in clinic or office (or ≥135/85 mm Hg at home) should be treated, aiming for a target diastolic BP of 85 mm Hg in the office (and systolic BP of 110–140 mm Hg) to reduce the likelihood of developing severe maternal hypertension and other complications, such as low platelets and elevated liver enzymes with symptoms. Antihypertensive drugs should be reduced or ceased if diastolic BP falls <80 mm Hg. Acceptable agents include oral methyldopa, labetalol, oxprenolol, and nifedipine, and second or third line agents include hydralazine and prazosin.
Women with preeclampsia should be assessed in hospital when first diagnosed; thereafter, some may be managed as outpatients once it is established that their condition is stable and they can be relied on to report problems and monitor their BP.
Women with preeclampsia who have proteinuria and severe hypertension, or hypertension with neurological signs or symptoms, should receive magnesium sulfate (MgSO4) for convulsion prophylaxis.
Fetal monitoring in preeclampsia should include an initial assessment to confirm fetal well-being. In the presence of fetal growth restriction, a recommended schedule for serial fetal surveillance with ultrasound is detailed within these recommendations.
Maternal monitoring in preeclampsia should include BP monitoring, repeated assessments for proteinuria if it is not already present, clinical assessment including clonus, and a minimum of twice weekly blood tests for hemoglobin, platelet count, and tests of liver and renal function, including uric acid, the latter being associated with worse maternal and fetal outcomes.
Women with preeclampsia should be delivered if they have reached 37 weeks’ (and zero days) gestation or if they develop any of the following:
Repeated episodes of severe hypertension despite maintenance treatment with 3 classes of antihypertensive agents;
Progressive thrombocytopenia;
Progressively abnormal renal or liver enzyme tests;
Pulmonary edema;
Abnormal neurological features, such as severe intractable headache, repeated visual scotomata, or convulsions;
Nonreassuring fetal status.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Postpartum Care
In the early postpartum period, women with preeclampsia should be considered at high risk for preeclamptic complications for at least 3 days and should have their BP and clinical condition monitored at least every 4 hours while awake. Antihypertensives administered antenatally should be continued, and consideration should be given to treating any hypertension before day 6 post-partum with antihypertensive therapy. Thereafter, antihypertensive therapy may be withdrawn slowly over days but not ceased abruptly. It is important to note that eclamptic seizures may develop for the first time in the early postpartum period.
Nonsteroidal anti-inflammatory drugs (NSAIDs) for postpartum analgesia should be avoided in women with preeclampsia unless other analgesics are not working; this is especially important if they have known renal disease, or preeclampsia is associated with placental abruption, AKI, or other known risk factors for AKI (eg, sepsis, postpartum hemorrhage).
All women should be reviewed at 3 months postpartum to ensure that BP, urinalysis, and any laboratory abnormalities have normalized. If proteinuria or hypertension persists, then appropriate referral for further investigations should be initiated.
There are significant long-term cardiovascular risks for women with chronic hypertension and those who have had gestational hypertension or preeclampsia. One initial recommendation may be to aim to achieve prepregnancy weight by 12 months and to limit interpregnancy weight gain through healthy lifestyle.
Annual medical review is advised life-long, and all such women should adopt a healthy lifestyle that includes exercise, eating well, and aiming for ideal body weight.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com


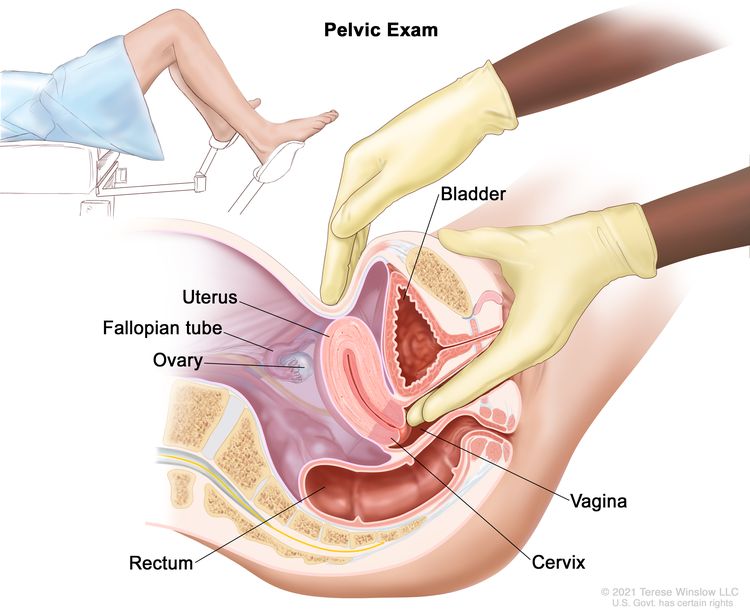 Pelvic exam. A doctor or nurse inserts one or two lubricated, gloved fingers of one hand into the vagina and presses on the lower abdomen with the other hand. This is done to feel the size, shape, and position of the uterus and ovaries. The vagina, cervix, fallopian tubes, and rectum are also checked.
Pelvic exam. A doctor or nurse inserts one or two lubricated, gloved fingers of one hand into the vagina and presses on the lower abdomen with the other hand. This is done to feel the size, shape, and position of the uterus and ovaries. The vagina, cervix, fallopian tubes, and rectum are also checked.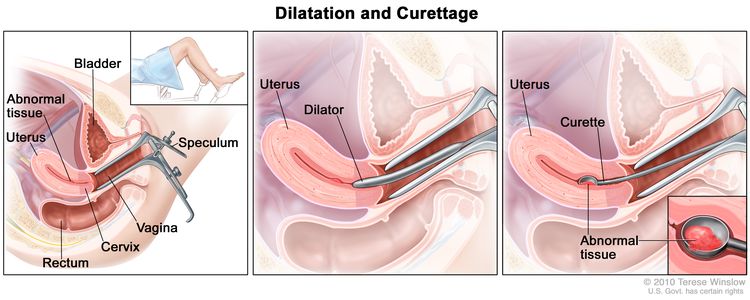 Dilatation and curettage (D and C). A speculum is inserted into the vagina to widen it in order to look at the cervix (first panel). A dilator is used to widen the cervix (middle panel). A curette is put through the cervix into the uterus to scrape out abnormal tissue (last panel).
Dilatation and curettage (D and C). A speculum is inserted into the vagina to widen it in order to look at the cervix (first panel). A dilator is used to widen the cervix (middle panel). A curette is put through the cervix into the uterus to scrape out abnormal tissue (last panel).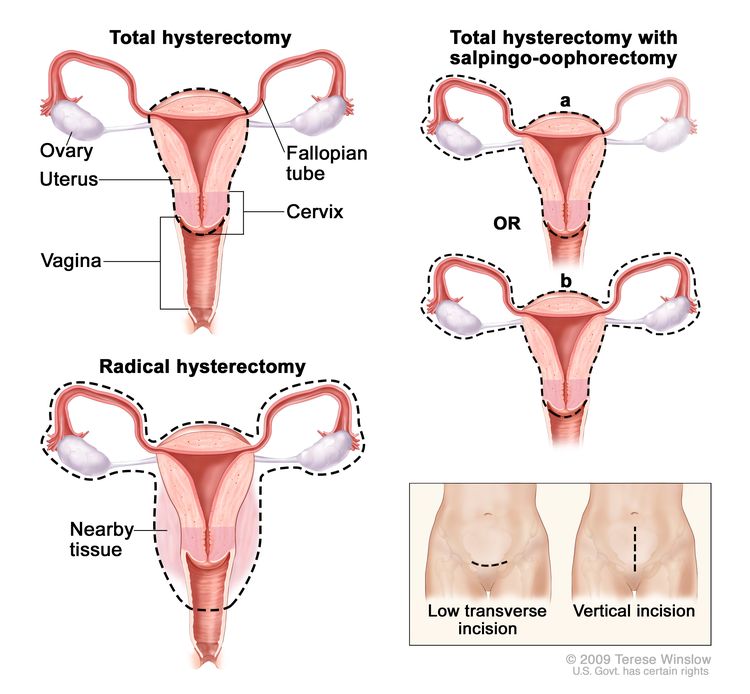 Hysterectomy. The uterus is surgically removed with or without other organs or tissues. In a total hysterectomy, the uterus and cervix are removed. In a total hysterectomy with salpingo-oophorectomy, (a) the uterus plus one (unilateral) ovary and fallopian tube are removed; or (b) the uterus plus both (bilateral) ovaries and fallopian tubes are removed. In a radical hysterectomy, the uterus, cervix, both ovaries, both fallopian tubes, and nearby tissue are removed. These procedures are done using a low transverse incision or a vertical incision.
Hysterectomy. The uterus is surgically removed with or without other organs or tissues. In a total hysterectomy, the uterus and cervix are removed. In a total hysterectomy with salpingo-oophorectomy, (a) the uterus plus one (unilateral) ovary and fallopian tube are removed; or (b) the uterus plus both (bilateral) ovaries and fallopian tubes are removed. In a radical hysterectomy, the uterus, cervix, both ovaries, both fallopian tubes, and nearby tissue are removed. These procedures are done using a low transverse incision or a vertical incision.


 Ultrasound
Ultrasound










