REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
From organizing your movie collection to deciding to buy a house, problem-solving makes up a large part of daily life. Problems can range from small (solving a single math equation on your homework assignment) to very large (planning your future career).
In cognitive psychology, the term problem-solving refers to the mental process that people go through to discover, analyze, and solve problems.1 The steps in the problem process include:
The discovery of the problem
The decision to tackle the issue
Understanding the problem
Researching the available options
Taking actions to achieve your goals
Before problem-solving can occur, it is important to first understand the exact nature of the problem itself. If your understanding of the issue is faulty, your attempts to resolve it will also be incorrect or flawed.
Problem-Solving Mental Processes
There are a number of mental processes at work during problem-solving. These include:
Perceptually recognizing a problem
Representing the problem in memory
Considering relevant information that applies to the current problem
Identify different aspects of the problem
Labeling and describing the problem
Problem-Solving Strategies
There are a number of different ways that people go about solving a problem. Some of these strategies might be used on their own, but people may also employ a range of approaches to figuring out and fixing a problem.
Algorithms
An algorithm is a step-by-step procedure that will always produce the correct solution. A mathematical formula is a good example of a problem-solving algorithm.
While an algorithm guarantees an accurate answer, it is not always the best approach to problem-solving.
This strategy is not practical for many situations because it can be so time-consuming. For example, if you were trying to figure out all of the possible number combinations to a lock using an algorithm, it would take a very long time.
Heuristics
A heuristic is a mental rule-of-thumb strategy that may or may not work in certain situations. Unlike algorithms, heuristics do not always guarantee a correct solution.
However, using this problem-solving strategy does allow people to simplify complex problems and reduce the total number of possible solutions to a more manageable set.2
Trial and Error
A trial-and-error approach to problem-solving involves trying a number of different solutions and ruling out those that do not work. This approach can be a good option if you have a very limited number of options available.
If there are many different choices, you are better off narrowing down the possible options using another problem-solving technique before attempting trial-and-error.
Insight
In some cases, the solution to a problem can appear as a sudden insight. This can occur because you realize that the problem is actually similar to something that you have dealt with in the past. However, the underlying mental processes that lead to insight happen outside of awareness.
Obstacles in Problem-Solving
Of course, problem-solving is not a flawless process. There are a number of different obstacles that can interfere with our ability to solve a problem quickly and efficiently. Researchers have described a number of these mental obstacles, which include functional fixedness, irrelevant information, and assumptions.
Assumptions: When dealing with a problem, people often make assumptions about the constraints and obstacles that prevent certain solutions.
Functional fixedness: This term refers to the tendency to view problems only in their customary manner.3 Functional fixedness prevents people from fully seeing all of the different options that might be available to find a solution.
Irrelevant or misleading information: When you are trying to solve a problem, it is important to distinguish between information that is relevant to the issue and irrelevant data that can lead to faulty solutions. When a problem is very complex, the easier it is to focus on misleading or irrelevant information.
Mental set: A mental set is the tendency people have to only use solutions that have worked in the past rather than looking for alternative ideas.4 A mental set can often work as a heuristic, making it a useful problem-solving tool. However, mental sets can also lead to inflexibility, making it more difficult to find effective solutions.
Define the Problem
The first step on problem solving is to define the problem- don’t skimp here because the problem may NOT be what you think it is! People often define problems in self-centered ways (“It’s about me!”) when the actual problem has little to do with them. For instance, if your partner forgets your birthday, you might think they don’t care as much for you as they once did, when it might really be about the partner being exhausted after working double shifts several days in a row. So, spend some time thinking about the circumstances of the problem before defining it. Also, be willing to re-define the problem as needed! Problems can be slippery things. A car mechanic has to take information from a customer as well as examining the car, both of which can give erroneous information! So she needs to adapt to new information. If the problem is with another person, that flexibility needs to be double. You’ll find a problem you thought you’d defined is really something else entirely.
One case study: June forgot Henry’s birthday. Henry initially thinks the issue relates to frustration with June’s unreliability, but if he thinks further, he might decide it is about how birthdays were the one place he felt special while growing up. The missed birthday brought back those feelings, and so he was upset at not at June, but at not feeling special. June’s actions were just a catalyst; it was really about the person’s feelings. Henry can’t expect June to know why birthdays mattered so much to him, unless he told her the story. And he might not even realize it himself until this situation happens, and he has to think about it!
Any sort of problem becomes easier once it is specified. Once you understand the kinds of math a word problem requires, it is just a matter of going through the steps!
2) Create your Solution, and Apply
Once the problem is specified, then a solution often becomes easier to find. In the Missed Birthday case, once Henry understands that the issue is about him feeling special, then he can talk to June about why events like birthdays matter. He may realize that talking about it makes it less important, and she does not need to change. He might say, “This is silly. I’m not twelve anymore, and I don’t need to be stuck on this anymore.” He might also decide it still matters, and they can then work on ways for her to do things that say to him, “You are special.” Knowing his feelings, she’s probably motivated to do more than just the birthday too. It might be telling him she appreciates how he contributes to their lives, for instance.
3) Review
A solution is only step 2. The last step is to check and see how the solution worked. In a math problem, you might check your work. In a problem that involves people, it would involve the person checking in with the other. So to go back to the Missing Birthday case, after a while Henry and June should check back in to see how they each feel about their solution.
Problems in Problem Solving
Most of the time, people solve problems fairly well. They get their needs met, they achieve their goals, and life is good. But there are the times when people don’t solve problems in good or accurate ways. They are not able to achieve their goals. Psychologists have found that there are typical patterns in the way people fail to solve problems correctly or accurately. There are two broad categories of these patterns. They are called Heuristics and Cognitive Biases.
Heuristics are estimates or educated guesses we use to solve a problem. At the grocery store, for example, you probably estimate how much you’ll spend to buy the items in your buggy. That estimate is a heuristic. When you see two people walking hand in hand and assume they are a couple, you’re using a heuristic. This method works “well enough” much of the time, and it saves a lot of time and energy. But there’s a problem when the heuristic doesn’t work, because then the person doesn’t meet their goals.
Cognitive Biases are tendencies or habits of mind that prevent people from solving a problem correctly. These biases can result in the person misrepresenting or even distorting their own experience or memory! A bias can be seen as like trying to roll a ball on a tilted floor. The ball will always tend to go “down” the tilt. Similarly, a cognitive bias tends to push thinking toward particular conclusions. For instance, a person who is a Democrat will tend to accept democratic ideas, candidates, etc, with less thinking and analysis than if looking at a Republican idea. The Democrat’s thinking is “tilted” toward Democratic ideas. This kind of bias is normal, and is fine as long as it is not so deeply rooted that it prevents the person from meeting their needs or goals.
Problem- a problem is anything that a person sets out to solve. It could involve figuring out the best choice for dinner, or troubleshooting a computer, or a disagreement between people. A “problem” can be a lot of things!
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Cognitive Biases
Confirmation bias-is a tendency for people to favor information that accords with their preconceptions regardless of the truth or strength of those claims. As a result, people gather evidence and recall information from memory selectively (Text). So someone who believes that their car is NOT reliable will tend to think about how often it has broken down, how much the breakdowns have cost, and so on, while minimizing or ignoring evidence to the contrary. They will actually be more likely to remember events, like the breakdowns, that confirm their belief and not recall all the times the car started and ran fine. As will all biases, this bias can mean that someone remembers one event over many, perhaps even dozens or hundreds of other events.
Attitude Polarization- This one describes a process where two people arguing take more extreme positions after the argument than before it. So their positions move apart instead of together.
Illusory Correlation- this bias refers to seeing relationships between events that don’t exist. One example is the relationship between cold weather and getting sick. Parents for generations have told children to wear their coats in the cold or they would get sick, but that is an illusion. Bacteria and viruses make people sick, not cold weather.
Overconfidence- the tendency to think we are better than we really are. This bias is good in that it gets us to try new things and attempt challenges. But it can be bad because it can lead to failure too. It is not well known, but the United States had a radar station in Hawaii on December 7, 1941, and that station picked up the Japanese aircraft as they approached Pearl Harbor to begin the surprise attack (MacDonald, n.d., Morgan, 1991). But the warning was ignored when they notified higher command. US commanders did not believe (overconfidence) that the Japanese could mount such an attack. Instead the officer concluded that the aircraft they saw had to be a flight of American planes coming in from the US mainland, even though they detected far more Japanese aircraft than the flight of six American planes they expected (MacDonald, n.d.; Morgan, 1991). Daniel Kahneman, one of the pioneers of this kind of research, has said that overconfidence is one of the most problematic of the biases, probably because it is so common.
Students sometimes confuse Overconfidence and Belief Perseveration. One difference is that Overconfidence is about the future; the overconfident person is overly optimistic about their ability to do something in the future. Someone showing Belief Perseveration is just about the belief continuing even in the face of evidence to disprove it.
Planning Fallacy- a special case of overconfidence, referring to people’s tendency to overestimate how much they can accomplish in a given time.
Framing- this is a bias in which the context, or lack of context, influences thinking. So a person who hears only that person A broke up with person B may think badly about person A. But with more context, it may be that person A really acted appropriately, such as if person B was abusive. What details and information are included about a situation have significant effects on a person’s thinking about that situation!
Belief Perseverance- this bias involves a person keeping to a belief even in the face of evidence to the contrary. Sometimes the evidence is overwhelming, but the person still holds to their belief. One example would be the “Flat Earth society” which still believes, based on a literal interpretation of the Bible, that the Earth is flat, despite all the evidence to the contrary.
Functional Fixedness- a special case of fixation, in which a person is unable to use an object for a purpose other than its “usual” purpose. For example a person needs a pointer, and has a pen. But they don’t use the pen because they can only see using the pen for writing.
Set Effect- a “Mental Set” is a subconsciously learned set of problem-solving techniques. Set effect is the tendency to use a mental set in solving new problems, and fail to solve the new problems correctly. The phrase, “If all you have is a hammer, everything starts to look like a nail” is an example. Another example- math problems can look similar, but require different techniques for solution. A person showing the Set Effect would try to solve new problems with the solutions they had learned for previous problems.
Heuristics
Representativeness- This heuristic involves making judgments about how likely something is to occur. When we encounter something new we tend to rely on what we’ve experienced before to make judgments about the new thing (Clause, 2015). The problem is that while the new thing might be like the previous, it might also be very different, and that can lead to errors in judgment, and bad decisions. Stereotyping can come from representativeness. If someone has an experience with a person of a group, and that person has little experience with that group, then they will tend to use the one experience to describe other members of that group. If that experience is bad, then this can create a negative stereotype.
Availability- This heuristic is a little complex. It involves us believing that certain events or actions are more common or more likely to occur than they really are. So a person believes that shark attacks are common even though they really are very rare. The process is that a person hears a lot about an event, and because they hear a lot about it, they can more easily remember information about it. That “ease of recall” leads people to believe that the event is more likely or common. So our person might hear news reports about a shark attack and think they happen all the time, when in reality they happen very very rarely. News encourages this kind of thinking, since rare events are what gets the most attention and reporting. As an example, there are many more news reports on airplane crashes than car crashes. Due to availability, people tend to think airplanes are more dangerous, even though cars are far more dangerous. like shark attacks. essentially means making decisions based on what comes to mind first.
Gambler’s Fallacy- this heuristic has to do with probability. It is the belief that if a random event has been occurring in a certain way, future events must change. So the gambler who has been losing at cards takes each loss as indication that the next time she’ll win. Of course, since the events are random, previous events have NO bearing on what happens in the future.
Anchoring and Adjustment- This heuristic is complicated, but in essence it indicates that the first piece of information a person receives about an object can set a person’s view of that object. So a person who doesn’t know about college tuition is looking at college costs. If they start looking at Harvard, then ODU will look cheap. If they start by looking at TCC, however, then ODU will look expensive! The first piece of information (the “Anchor”) will set the sense of “normal” and people’s thinking will change as a result. After being “anchored” the person will use it as the point from which they consider other events. If the person exposed to Harvard tuition was asked about what was reasonable college tuition, they would “adjust” from Harvard tuition, and give a higher number than the person exposed to ODU tuition instead.
Escalation of Commitment- involves a person, once making an initial effort or contribution to some effort, making more contributions because of the first one. This is often used to justify increased commitment in wars- a politician will say something about how our sacrifices would be in vain if we withdrew now, and that we should commit more to the war. This heuristic is separate from the validity of the effort in question; the problem comes out of using the initial investment as justification for more investment. The problem is that the new investment may turn out just as badly as the previous one. In those committing this fallacy, now the two commitments both “justify” another, and another, and so on. This can lead to far greater losses than had the person gotten out in the first place.
Familiarity- this heuristic refers to a person examining a new problem, seeing it as like a previous problem, and using the solution from the previous problem for the new one. The person doesn’t notice the differences between the old and new problems, and it is easy for them to retrieve the old solution. The new problem, however, may not be enough alike the old one for the solution to work.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Cognition is a term referring to the mental processes involved in gaining knowledge and comprehension. These cognitive processes include thinking, knowing, remembering, judging, and problem-solving.1 These are higher-level functions of the brain and encompass language, imagination, perception, and planning.
Cognitive psychology is the field of psychology that investigates how people think and the processes involved in cognition.
Types of Cognitive Processes
There are many different types of cognitive processes. These include:
Attention: Attention is a cognitive process that allows people to focus on a specific stimulus in the environment.
Language: Language and language development are cognitive processes that involve the ability to understand and express thoughts through spoken and written words. It allows us to communicate with others and plays an important role in thought.
Learning: Learning requires cognitive processes involved in taking in new things, synthesizing information, and integrating it with prior knowledge.
Memory:Memory is an important cognitive process that allows people to encode, store, and retrieve information. It is a critical component in the learning process and allows people to retain knowledge about the world and their personal histories.
Perception: Perception is a cognitive process that allows people to take in information through their senses (sensation) and then utilize this information to respond and interact with the world.
Thought:Thought is an essential part of every cognitive process. It allows people to engage in decision-making, problem-solving, and higher reasoning.
Uses
Cognitive processes affect every aspect of life, from school to work to relationships. Some specific uses for these cognitive processes include the following.
Learning New Things
Learning requires being able to take in new information, form new memories, and make connections with other things that you already know. Researchers and educators use their knowledge of these cognitive processes to help create instructive materials to help people learn new concepts.
Forming Memories
Memory is a major topic of interest in the field of cognitive psychology. How we remember, what we remember, and what we forget reveal a great deal about how the cognitive processes operate.
While people often think of memory as being much like a video camera, carefully recording and cataloging life events, and storing them away for later recall, research has found that memory is much more complex.
Making Decisions
Whenever people make any type of decision, it involves making judgments about things they have processed. It might involve comparing new information to prior knowledge, integrating new information into existing ideas, or even replacing old knowledge with new knowledge before making a choice.
Impact of Cognition
The cognitive processes have a wide-ranging impact that influences everything from daily life to overall health.
Perceiving the World
As you take in sensations from the world around you, the information that you see, hear, taste, touch, and smell must first be transformed into signals that your brain can understand. The perceptual process allows you to take in sensory information and convert it into a signal that your brain can understand and act upon.2
Forming Impressions
The world is full of an endless amount of sensory experiences. To make meaning out of all this incoming information, it is important for your brain to be able to reduce your experience of the world down to the fundamentals. You remember everything, so events are reduced down to the critical concepts and ideas that you need.3
Filling in the Gaps
In addition to reducing information to make it more memorable and understandable, people also elaborate on these memories as they reconstruct them. In some cases, this elaboration happens when people are struggling to remember something. When the information cannot be recalled, the brain sometimes fills in the missing data with whatever seems to fit.4
Interacting With the World
Cognition involves not only the things that go on inside our heads but also how these thoughts and mental processes influence our actions.5 Our attention to the world around us, memories of past events, understanding of language, judgments about how the world works, and abilities to solve problems all contribute to how we behave and interact with our surrounding environment.
Cognitive Processes
What are cognitive processes? We can understand cognitive processes as the procedures we use to incorporate new knowledge and make decisions based on said knowledge. Different cognitive functions play a role in these cognitive processes: perception, attention, memory, reasoning… Each of these cognitive functions work together to integrate the new knowledge and create an interpretation of the world around us.
ATTENTION AS A COGNITIVE PROCESS: Attention is the cognitive process that allows us to concentrate on a stimuli or activity in order to process it more thoroughly later. Attention is a fundamental cognitive function for the development of daily situations, and it is used in the majority of tasks that we carry-out day-to-day. In fact, it has been considered a mechanism that controls and regulates the rest of the cognitive processes: from perception (we need attention to be able to pay attention to the stimuli that don’t reach our senses) to learning and complex reasoning.
MEMORY AS A COGNITIVE PROCESS: Memory is the cognitive function that allows us to code, store, and recover information from the past. Memory is a basic process for learning, as it is what allows us to create a sense of identity. There are many types of memory, like short-term memory, which is the ability to retain information for a short period of time (remember a telephone number until we can write it down on paper), and long-term memory, which are all of the memories that we keep for a long period of time. Long-term memory can be broken into smaller groups, declarative memory and procedural memory. Declarative memory consists of the knowledge that was acquired through language and education (like knowing that World War II ended in 1945), as well as knowledge learned through personal experiences (remembering what my grandma used to make for me). Procedural memory refers to learning though routines (learning how to drive or ride a bike). Other types of memory are auditory memory, contextual memory, naming, and recognition.
PERCEPTION AS A COGNITIVE PROCESS: Cognitive perception allows us to organize and understand the world through stimuli that we receive from our different senses, like sight, hearing, taste, smell, and touch. While most people are familiar with the common senses, there are some other, less-known senses, like propioception (stimuli which unconsciously perceives our position in space and judges spatial orientation) and interoception (which is the perception of our organs in our bodies. It is what allows us to know when we’re hungry or thirsty). Once the stimuli is received, our brain integrates all of the information, creating a new memory.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
LANGUAGE AS A COGNITIVE PROCESS: Language is the ability to express our thoughts and feelings through spoken word. It is a tool that we use to communicate and organize and transmit information that we have about ourselves and the world. Language and thought are developed together and are closely related, they mutually influence each other.
THOUGHT AS A COGNITIVE PROCESS: Thought is fundamental for all cognitive processes. It allows us to integrate all of the information that we’ve received and to establish relationships between events and knowledge. To do this, it uses reasoning, synthesis, and problem solving (executive functions).
LEARNING AS A COGNITIVE PROCESS: Learning is the cognitive process that we use to incorporate new information into our prior knowledge. Learning includes things as diverse as behaviors or habits, like brushing our teeth or learning how to walk, and knowledge that we learn through socialization. Piaget and other authors have talked about cognitive learning as the process of information entering our cognitive system and changing it.
The cognitive processes can happen naturally or artificially, consciously or unconsciously, but they usually happen fast. These cognitive processes work constantly and without us realizing them. For example, when we are walking on the street and we see a stoplight turn red, we start the cognitive process that tells us to make a decision (cross or don’t cross). The first thing that we do is focus our attention on the stoplight, through our sight we can see that it is red. In just milliseconds, we recall from our memory that when the stoplight is red you shouldn’t cross. This is probably where we make our first decision: wait until the light turns green, or look right and left (shifting our attention again) to see if any cars are coming and make the decision to cross quickly.
Tips
Cognitive processes are influenced by a range of factors including genetics and experiences. While you cannot change your genetics, there are things that you can do to protect and maximize your cognitive abilities:
Stay healthy. Lifestyle factors such as eating healthy and getting regular exercise can have an effect on your cognitive functioning.
Think critically. Question your assumptions and ask questions about your thoughts, beliefs, and conclusions.
Stay curious and keep learning. One great way to flex your cognitive abilities is to keep challenging yourself to learn more about the world.
Skip multitasking. While it might seem like doing several things at once would help you get done faster, research has shown it actually decreases both productivity and work quality.
The Cognitive and Productive Costs of Multitasking
Potential Pitfalls
It is important to remember that these cognitive processes are complex and often imperfect. Some of the possible pitfalls that can affect cognition include:
Problems with attention: Selective attention is a limited resource, so there are a number of things that can make it difficult to focus on everything in your environment. Attentional blink, for example, happens when you are so focused on one thing that you completely miss something else happening right in front of you.
Memory problems and limitations: Short-term memory is surprisingly brief, typically lasting just 20 to 30 seconds.6 Long-term memory can be surprisingly stable and enduring, on the other hand, with memories lasting years and even decades.7 Memory can also be surprisingly fragile and fallible. Sometimes we forget, and other times we are subject to misinformation effects that can even lead to the formation of false memories.8
Cognitive biases: Cognitive biases are systematic errors in thinking related to how people process and interpret information about the world. The confirmation bias is one common example that involves only paying attention to information that aligns with your existing beliefs while ignoring evidence that doesn’t support your views.
Types of Cognitive Biases
History of the Study of Cognition
The study of how we think dates back to the time of the ancient Greek philosophers Plato and Aristotle.
Philosophical Origins
Plato’s approach to the study of the mind suggested that people understand the world by first identifying basic principles buried deep inside themselves and then using rational thought to create knowledge. This viewpoint was later advocated by philosophers such as Rene Descartes and linguist Noam Chomsky. This approach to cognition is often referred to as rationalism.9
Aristotle, on the other hand, believed that people acquire their knowledge through their observations of the world around them. Later thinkers including John Locke and B.F. Skinner also advocated this point of view, which is often referred to as empiricism.10
Early Psychology
During the earliest days of psychology and for the first half of the twentieth century, psychology was largely dominated by psychoanalysis, behaviorism, and humanism. Eventually, a formal field of study devoted solely to the study of cognition emerged as part of the “cognitive revolution” of the 1960s. The field of psychology concerned with the study of cognition is known as cognitive psychology.
The Emergence of Cognitive Psychology
One of the earliest definitions of cognition was presented in the first textbook on cognitive psychology published in 1967. According to Neisser, cognition is “those processes by which the sensory input is transformed, reduced, elaborated, stored, recovered, and used.”
Can You Improve Cognition?
Is it possible to improve cognition? Below is a tool oriented to improve cognition and cognitive performance:
THE COGNITIVE STIMULATION PROGRAM FROM COGNIFIT: This program was designed by a team of neurologists and cognitive psychologists that study synaptic plasticity and neurogenesis processes. You only need 15 minutes a day (2-3 times a week) to stimulate your cognition. This program is available online, and has specific programs for personal use, researchers, health professionals, and schools.
The cognitive stimulation exercises from CogniFit effectively assess more than 20 fundamental cognitive functions, which are clearly defined and subject to an objective target control, which provides standardized results of age and demographic criteria based on thousands of results.
The different interactive exercises are presented as fun brain games that you can practice on your computer. After each session, CogniFit will present a detailed picture, showing the evolution of the user’s cognitive state. It also compares their cognitive performance to other users.
If neuroscience and studying brain plasticity has shown us anything, it is that the more we use a neural circuit, the stronger it gets. The cognitive stimulation program from CogniFit works to explore our cognitive processes. Once we are able to understand each individual’s cognitive state, we are offer them a personalized cognitive training program. Focusing on the most challenging tasks will ensure that we are creating and establishing new neural connections, which will get stronger and stronger the more that they are trained.
REDUCE STRESS LEVEL: Stress increases cortisol levels, which attacks the myelin of the axons and impedes information from being efficiently transmitted. If we are able to reduce the stress in our lives, we may be able to improve our cognition, because reducing stress improves synaptic connections. Keeping a positive attitude makes us more creative when solving problems, and probably makes us more cognitively flexible.
MEDITATION: Meditation can also help our cognition. In the last few years, more and more studies have been looking at the effects of meditation on cognitive processes. It requires concentration and conscious attention, which as we said, are important for creating new functional circuits. The study seems to support this idea, and meditation has been related to improvements in attention, memory, executive functions, processing speed, and general cognition.
PHYSICAL EXERCISE: Doing some exercise can also improve it. It doesn’t need to be particularly intense activities. In fact, walking 45 minutes, 3 times a week seems to improve memory and reasoning (executive functions), and practicing Tai-Chi improves mainly executive functioning.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Learning involves a change in behavior or knowledge that results from experience.
The word learning is used routinely in discussions about teaching in higher education, so it’s important to clarify what we are referring to when we talk about learning. Educational researchers agree that learning is much deeper than memorization and information recall. Deep and long-lasting learning involves understanding, relating ideas and making connections between prior and new knowledge, independent and critical thinking and ability to transfer knowledge to new and different contexts.
Psychologists often define learning as a relatively permanent change in behavior as a result of experience. The psychology of learning focuses on a range of topics related to how people learn and interact with their environments.
One of the first thinkers to study how learning influences behavior was psychologist John B. Watson who suggested that all behaviors are a result of the learning process. The school of thought that emerged from Watson’s work was known as behaviorism. The behavioral school of thought proposed studying internal thoughts, memories, and other mental processes that were too subjective.
Psychology, the behaviorists believed, should be the scientific study of observable behavior. Behaviorism thrived during the first half of the twentieth century and contributed a great deal to our understanding of some important learning processes.
Are you preparing for a big test in your psychology of learning class? Or are you just interested in a review of learning and behavioral psychology topics? This learning study guide offers a brief overview of some of the major learning issues including behaviorism, classical, and operant conditioning.
Let’s learn a bit more about the psychology of learning.
Learning
Learning can be defined in many ways, but most psychologists would agree that it is a relatively permanent change in behavior that results from experience. During the first half of the twentieth century, the school of thought known as behaviorism rose to dominate psychology and sought to explain the learning process.
The three major types of learning described by behavioral psychology are classical conditioning, operant conditioning, and observational learning.
Behaviorism
Behaviorism was the school of thought in psychology that sought to measure only observable behaviors.
Founded by John B. Watson and outlined in his seminal 1913 paper Psychology as the Behaviorist Views It, the behaviorist standpoint held that psychology was an experimental and objective science and that internal mental processes should not be considered because they could not be directly observed and measured.
Watson’s work included the famous Little Albert experiment in which he conditioned a small child to fear a white rat. Behaviorism dominated psychology for much of the early twentieth century. While behavioral approaches remain important today, the latter part of the century was marked by the emergence of humanistic psychology, biological psychology, and cognitive psychology.
Types of Learning
There are three main types of learning: classical conditioning, operant conditioning, and observational learning. Both classical and operant conditioning are forms of associative learning, in which associations are made between events that occur together. Observational learning is just as it sounds: learning by observing others.
Classical Conditioning
Classical conditioning is a process by which we learn to associate events, or stimuli, that frequently happen together; as a result of this, we learn to anticipate events. Ivan Pavlov conducted a famous study involving dogs in which he trained (or conditioned) the dogs to associate the sound of a bell with the presence of a piece of meat. The conditioning is achieved when the sound of the bell on its own makes the dog salivate in anticipation for the meat.
Imagine your favorite snack is peanut butter and jelly sandwiches. Whenever you get that snack, it makes you happy and you start to jump around, doing your happy PB&J dance. Your sandwich always comes on the same plate – it’s big and orange and has a picture of a tiger on it. Eventually, you might start doing your PB&J dance whenever you see your tiger plate on the table, in anticipation of the sandwich arriving.
Cartoon explaining what classical conditioning is. This type of conditioning is called classical conditioning. The presence of the plate has caused you to have the same reaction as having a PB&J sandwich. The sandwich is our stimulus (the unconditioned stimulus) and it elicits the dance which is our response (the unconditioned response). “Unconditioned” refers to the fact that no learning took place to connect the stimulus and response – you saw the the sandwich and automatically got so excited you start to dance (like a reflex!).
Cartoon explaining what an unconditioned response is as well as a neutral stimulus. The plate starts off as a neutral stimulus and elicits no reaction on its own. As it is continuously paired with the sandwich, the plate becomes a conditioned stimulus and elicits a conditioned response in the form of your happy dance. Over time, you have learned to connect the plate and the feelings of happiness that cause you to dance.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Cartoon showing how the tiger plate turns from a neutral stimulus to a conditioned stimulus over time. Also interesting to think about is just why it is you dance when you see that sandwich in the first place. Earlier, we stated that it is was the unconditioned stimulus because it took no learning to cause you to dance at the sight of it. At the start of our thought experiment, that was true. However, when you were first introduced to PB&J, you would dance while eating it because it tasted so good. Eventually, an association between sight and taste formed (learned via classical conditioning) and you began to dance preemptively – just the sight was enough to trigger the feelings of joy expressed by the dance.. If we really follow this line of thought about our everyday actions, we’ll find that many, if not most, of our actions can be traced back to pretty basic needs like food, shelter, comfort, etc.
Operant Conditioning
Operant conditioning is the learning process by which behaviors are reinforced or punished, thus strengthening or extinguishing a response. Edward Thorndike coined the term “law of effect,” in which behaviors that are followed by consequences that are satisfying to the organism are more likely to be repeated, and behaviors that are followed by unpleasant consequences are less likely to be repeated. B. F. Skinner researched operant conditioning by conducting experiments with rats in what he called a “Skinner box.” Over time, the rats learned that stepping on the lever directly caused the release of food, demonstrating that behavior can be influenced by rewards or punishments. He differentiated between positive and negative reinforcement, and also explored the concept of extinction.
In classical conditioning, the stimuli that precede a behavior will vary (PB&J sandwich, then tiger plate), to alter that behavior(e.g. dancing with the tiger plate!). In operant conditioning, the consequences which come after a behavior will vary, to alter that behavior. Imagine years down the road you are still enamored of delicious PB&J sandwiches, and now are trying to teach yourself to be a good roommate. The house rule is that whoever leaves their dishes unwashed the longest has to take out the trash. You hate taking out the trash, so you develop a system – whenever you remember to wash your plate, you are allowed to surf the internet, otherwise you’re not allowed. The more dishes you wash, the more you get to procrastinate on your favorite sites. Initially, you leave the plate in the sink a few times, then you begin to remember after a day or so, and finally you start to wash your dishes immediately after using them. This process of shaping involves intermediate behaviors (leaving the plate in the sink and beginning to come back to wash the dishes within hours) that start moving you towards the goal behavior (washing your dishes immediately).
Observational Learning
Observational learning occurs through observing the behaviors of others and imitating those behaviors—even if there is no reinforcement at the time. Albert Bandura noticed that children often learn through imitating adults, and he tested his theory using his famous Bobo-doll experiment. Through this experiment, Bandura learned that children would attack the Bobo doll after viewing adults hitting the doll.
How do we influence behavior?
Operant conditioning changes behaviors by using consequences, and these consequences will have two characteristics:
Reinforcement or punishment
–Reinforcement is a response or consequence that causes a behavior to occur with greater frequency.-Punishment is a response or consequence that causes a behavior to occur with less frequency.
Positive or negative
–Positive means adding a new stimulus.-Negative means removing an old stimulus. There end up being 4 different ways we can affect behavior with operant conditioning:
negative reinforcement
–
positive reinforcement
negative punishment
–
positive punishment
Let’s go back to our example of washing the dishes, and consider the four different types of operant conditioning based consequences. If you leave the dish on the table instead of washing it, some sort of punishment will happen because this is an undesired behavior.
Positive punishment: You will get a new chore such as sweeping the floors! (adding a new stimulus).
Negative punishment: You will not get to eat the usual apple pie dessert (removing an old stimulus)
If you remember to wash your plate, some sort of reinforcement will happen because this is a desired behavior.
Positive reinforcement: You will get to make one online purchase! (adding a new stimulus).
Negative reinforcement: You won’t have to take out the trash this week, a standard chore (removing an old stimulus).
How effective is the conditioning?
Imagine your tiger plate was one of a set of plates – jungle cat plates. There is a lion, a jaguar, and a leopard as well
Cartoon showing the different types of animal plates in the set.They’re all generally the same shape and color, so you react to these plates the same way you reacted to the tiger plate, (the original conditioned stimulus) and do your happy dance. We call this generalization – when a conditioned response (happy dance) occurs in reaction to a stimulus (jungle cat plates) other than (but often similar to) the conditioned one (tiger plate). A good way to remember is that now you do a happy dance for cat plates in general. The opposite of generalization is discrimination – the ability to tell different stimuli apart and react only to certain ones. You show discrimination whenever you don’t dance because you can tell the difference between the peanut butter and the pickle jars, for example, or by dancing only at snack time, since you know that’s the only time the PB&J happens. Imagine that you’ve run out of peanut butter, so you’re stuck with tuna salad for weeks (oh no!). Your parents try to make it better by serving it on your favorite tiger plate, but you soon realize the tiger plate does not mean PB&J. You lose the association between the tiger plate and PB&J, and stop doing your happy dance whenever you see that plate. We call this extinction – your conditioned response (happy dance) disappeared. However, when peanut butter in your house again and your parents serve you PB&J on your tiger plate, the previous association between the tiger plate and PB&J dance quickly will come back in full force. We call this spontaneous recovery.While the discussion above focused on our examples from classical conditioning, the same concepts can be applied to operant conditioning as well. Maybe your chore scheme works so well you begin to wipe down the kitchen counters whenever you make a big meal, or you refuse to allow yourself pie if you haven’t folded your laundry.
What are examples of conditioning in your daily life?
Conditioning, both classical and operant, can be seen throughout our daily lives. Insurance companies will charge you more if you keep getting into accidents (negative punishment) or give you congratulatory certificates for safer driving (positive reinforcement). When driving, seeing flashing lights in your rearview mirror coupled with a siren will cause a gut feeling of dread even before the officer comes by with your ticket. Maybe it’s not even you they’re pulling over, but those signals (conditioned stimuli) are so associated with tickets and fines (unconditioned stimuli) that you can feel it in your stomach (conditioned response). Now that we’ve explored conditioning some, be on the lookout for examples in your day to day life, and maybe even consider using some of those techniques on yourself – for every hour and a half of studying, give yourself a ten minute break to stretch and watch funny videos or walk around!
Key Points
Learning involves physical changes in the nervous system, such as the strengthening of synapses, the activation of neural pathways, or the pruning of neural pathways. These changes elicit specific responses to environmental stimuli.
The field of behavioral psychology focuses largely on measurable behaviors that are learned, rather than trying to understand internal states such as emotions and attitudes.
Types of learning include classical and operant conditioning (both forms of associative learning) as well as observational learning.
Classical conditioning, initially described by Ivan Pavlov, occurs when a particular response to a stimulus becomes conditioned to respond to another associated stimulus.
Operant conditioning, initially described by B. F. Skinner, is the learning process by which a response is strengthened or extinguished through the reinforcement or punishment of a behavior.
Observational learning, initially described by Albert Bandura, occurs through observing the behaviors of others and imitating those behaviors, even if there is no reinforcement at the time.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Emotions can play an important role in how we think and behave. The emotions we feel each day can compel us to take action and influence the decisions we make about our lives, both large and small. In order to truly understand emotions, it is important to understand the three critical components of an emotion.
There are three parts to an emotion:
A subjective component (how you experience the emotion)
A physiological component (how your bodies react to the emotion)
An expressive component (how you behave in response to the emotion).
These different elements can play a role in the function and purpose of your emotional responses.
Emotions can be short-lived, such as a flash of annoyance at a co-worker, or long-lasting, such as enduring sadness over the loss of a relationship. But why exactly do we experience emotions? What role do they serve?
For starters, it’s not the same thing as mental health. While the two terms are often used interchangeably, emotional health “focuses on being in tune with our emotions, vulnerability, and authenticity,” says licensed psychologist Juli Fraga, PsyD.
Having good emotional health is a fundamental aspect of fostering resilience, self-awareness, and overall contentment.
Keep in mind that having good emotional health doesn’t mean you’re always happy or free from negative emotions. It’s about having the skills and resources to manage the ups and downs of day-to-day life.
How does it look in action?
Here’s a look at some common examples of good emotional health and the impact it can have.
1. Noticing upsetting emotions when they arise
This enables you to name them and process them in healthy ways. For example, you might choose to compassionately confront someone who hurt or angered you rather than lash out at them. Or maybe you opt to set some healthy boundaries at work or with loved ones.
2. Catching your own self-judgments
According to Fraga, this means turning that critical inner voice into an opportunity for self-love and compassion.
For example, when you find yourself engaging in negative self-talk, you might ask:
“If my child, partner, or best friend were talking to me this way, how would I respond?”
“What makes it challenging for me to treat myself the same way I treat others?”
3. Curiosity
Emotional health flourishes when you’re curious about your thoughts, behaviors, and feelings and why they might arise at certain times, says Fraga.
It’s important to be able to ask yourself, “Why do I react this way?” or “What is it about my past that might lead me to have a strong reaction to x, y, and z?”
Why is it so important?
Working on our emotional health is just as important as taking care of our physical well-being.
And that work pays off with:
Resilience to stress. ResearchTrusted Source shows that emotional distress makes you more vulnerable to physical illness by impacting your immune system.
Deeper relationships. When you’re equipped with the skills to manage your emotions, it’s easier for you to connect with others and show more empathy and compassion. You’re also better able to hold arguments and talk through your feelings.
Higher self-esteem. Your thoughts, feelings, and experiences influence the way you feel about yourself. Good emotional health helps you see the best in yourself despite challenges.
More energy. Having a positive outlook makes you feel more energized and helps you focus and think more clearly, whereas poor emotional health depletes your mental resources and leads to exhaustion.
How can I improve my emotional health?
Emotional health is more of a process than a goal. And chances are you’re already doing some things that help strengthen your emotional health.
As you go through these tips, remember that emotional health isn’t about always being in a good mood. It’s about equipping yourself to deal with the good, the bad, and everything in between.
1. Practice emotional regulation
Emotions can and sometimes will get the best of you, but learning coping strategies to temper them can help you respond instead of react to upsetting situations, Fraga advises.
Coping strategies can include:
meditation
journaling
listening to music
talking to a therapist
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
2. Exercise
If you’re overwhelmed with stress at work or at home, getting regular exercise can feel impossible. But taking the time for physical activity can nourish both your emotional and your physical health, says Fraga.
Aim to set aside 30 minutes a day for some kind of physical activity. If you’re short on time, find 10- or 15-minute chunks of time to go for a quick walk.
3. Strengthen social connections
Your links to others can have powerful effects on your emotional and physical health. Staying connected with loved ones can provide a buffer when you’re going through challenges,
Foster these connections by spending time with close friends and family, either in person or over the phone.
4. Be mindful
A growing body of research links mindfulness with less emotional reactivity and greater relationship satisfaction.
Mindfulness can be as simple as focusing on one thing at a time, trying a social media detox, or turning household tasks into a mental break. The point is to be consistent with your mindfulness practice and dedicate even just a few minutes to something you enjoy.
5. Get quality sleep
Sacrificing sleep makes you more vulnerable to stress and anxiety.
One 2018 study found that being sleep-deprived leads to more repetitive negative thoughts. Being overly tired can make you more emotionally reactive. That emotional reactivity can negatively affect your outlook, performance, and relationships.
Make sure you’re being consistent with your sleep and waking times as well as optimizing your bedroom environment so that you’re getting enough rest.
The bottom line
Good emotional health is crucial to your overall well-being. If you feel like your thoughts and emotions are getting the best of you, taking care of your core needs — like sleep and connection with loves ones — can help.
If that doesn’t seem to do the trick, consider working with a therapist or another mental health professional. They can help you clearly identify the aspects of your emotional health you want to improve and help you come up with a plan.
Emotions Can Motivate Us to Take Action
When faced with a nerve-wracking exam, you might feel a lot of anxiety about whether you will perform well and how the test will impact your final grade. Because of these emotional responses, you might be more likely to study. Since you experienced a particular emotion, you had the motivation to take action and do something positive to improve your chances of getting a good grade.
We also tend to take certain actions in order to experience positive emotions and minimize the probability of feeling negative emotions. For example, you might seek out social activities or hobbies that provide you with a sense of happiness, contentment, and excitement. On the other hand, you would probably avoid situations that might potentially lead to boredom, sadness, or anxiety. 5 Surprising Ways to Increase Motivation
Emotions Help Us Survive, Thrive, and Avoid Danger
Naturalist Charles Darwin believed that emotions are adaptations that allow both humans and animals to survive and reproduce. When we are angry, we are likely to confront the source of our irritation. When we experience fear, we are more likely to flee the threat. When we feel love, we might seek out a mate and reproduce.
Emotions serve an adaptive role in our lives by motivating us to act quickly and take actions that will maximize our chances of survival and success.
Emotions Can Help Us Make Decisions
Our emotions have a major influence on the decisions we make, from what we decide to have for breakfast to which candidates we choose to vote for in political elections. Researchers have also found that people with certain types of brain damage affecting their ability to experience emotions also have a decreased ability to make good decisions.
Even in situations where we believe our decisions are guided purely by logic and rationality, emotions play a key role. Emotional intelligence, or our ability to understand and manage emotions, has been shown to play an important role in decision-making. 5 Reasons Why We Make Bad Decisions
Emotions Allow Other People to Understand Us
When we interact with other people, it is important to give clues to help them understand how we are feeling. These cues might involve emotional expression through body language, such as various facial expressions connected with the particular emotions we are experiencing.
In other cases, it might involve directly stating how we feel. When we tell friends or family members that we are feeling happy, sad, excited, or frightened, we are giving them important information that they can then use to take action.
Emotions Allow Us to Understand Others
Just as our own emotions provide valuable information to others, the emotional expressions of those around us give us a wealth of social information. Social communication is an important part of our daily lives and relationships, and being able to interpret and react to the emotions of others is essential.
It allows us to respond appropriately and build deeper, more meaningful relationships with our friends, family, and loved ones. It also allows us to communicate effectively in a variety of social situations, from dealing with an irate customer to managing a hot-headed employee.
Charles Darwin was one of the earliest researchers to scientifically study emotions. He suggested that emotional displays could also play an important role in safety and survival. If you encountered a hissing or spitting animal, it would clearly indicate that the creature was angry and defensive, leading to you back off and avoid possible danger.
Understanding the emotional displays of others gives us clear information about how we might need to respond in a particular situation.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Motivation is the desire to act in service of a goal. It’s the crucial element in setting and attaining our objectives.
Motivation is one of the driving forces behind human behavior. It fuels competition and sparks social connection. Its absence can lead to mental illnesses such as depression. Motivation encompasses the desire to continue striving toward meaning, purpose, and a life worth living.
Motivation is the process that initiates, guides, and maintains goal-oriented behaviors. It is what causes you to act, whether it is getting a glass of water to reduce thirst or reading a book to gain knowledge.
Motivation involves the biological, emotional, social, and cognitive forces that activate behavior. In everyday usage, the term “motivation” is frequently used to describe why a person does something. It is the driving force behind human actions.
Motivation doesn’t just refer to the factors that activate behaviors; it also involves the factors that direct and maintain these goal-directed actions (though such motives are rarely directly observable). As a result, we often have to infer the reasons why people do the things that they do based on observable behaviors.1
What exactly lies behind the motivations for why we act? Psychologists have proposed different theories of motivation, including drive theory, instinct theory, and humanistic theory (such as Maslow’s hierarchy of needs). The reality is that there are many different forces that guide and direct our motivations.
Motivation Definition in Psychology
The study of motivation in psychology revolves around providing the best possible answers to two fundamental questions: what causes behavior, and why does behavior vary in its intensity?
Motivational science is a behavioral science that seeks to construct theories about what constitutes human motivation and how motivational processes work.
Motivation, when seen in the real world, and when measured by science, becomes visible and detectable through behavior, level of engagement, neural activation, and psychophysiology. Some would also include self-report in this list, but studies show that self-reports have proven to be highly unreliable sources of information.
Types of Motivation
Different types of motivation are frequently described as being either extrinsic or intrinsic:
Extrinsic motivations are those that arise from outside of the individual and often involve rewards such as trophies, money, social recognition, or praise.
Intrinsic motivations are those that arise from within the individual, such as doing a complicated crossword puzzle purely for the personal gratification of solving a problem.
Reasons to Exercise
Type of Motivation
Real-Life Examples
Fun, enjoyment
Intrinsic motivation
Children run, jump, and chase simply for the sheer fun of it.
Personal challenge
Flow
Performers get “in the zone” when their pursuits optimally challenge their skills.
Forced to do so
External regulation
Athletes exercise because their coach tells them to do so.
Accomplish a goal
Goal
Runners strive to run a mile in six minutes or less.
Health benefits
Value
Patients exercise to lose weight or to strengthen the heart.
Inspiration
Possible self
People watch others exercise and become inspired to do the same.
Pursuit of a standard of excellence
Achievement strivings
Snow skiers race to the bottom of the mountain, trying to beat their previous best time.
Satisfaction from a job well done
Competence
As exercisers make progress, they feel more competent, more effective.
An emotional kick
Opponent process
Vigorous jogging can produce a runner’s high, a euphoric rebound to the pain.
Good mood
Positive affect
Being in nature can induce a good mood such that people exercise spontaneously, skipping along without even knowing why.
Alleviate guilt
Introjection
People exercise because they think that is what they should or ought to do to please others or to relieve their sense of guilt.
Relieve stress and anxiety
Personal control
After a stressful day, people go to the gym, which they see as a structured and controllable environment.
Spend time with friends
Relatedness
Exercise is often a social event, a time to enjoy hanging out with friends.
Sources of Motivation
People often have multiple motives for engaging in any one behavior. Motivation might be extrinsic, whereby a person is inspired by outside forces—other people or rewards. Motivation can also be intrinsic, whereby the inspiration comes from within—the desire to improve at a certain activity. Intrinsic motivation tends to push people more forcefully, and the accomplishments are more fulfilling.
One framework used for understanding motivation is the hierarchy of needs proposed by American psychologist Abraham Maslow in 1943. According to Maslow, humans are inherently motivated to better themselves and move toward expressing their full potential—self-actualization—by progressively encountering and satisfying several levels of need from the most fundamental, such as for food and safety, to higher-order needs for love, belonging, and self-esteem.
Eventually, Maslow extended the theory to include a need for self-transcendence: People reach the pinnacle of growth and find the highest meaning in life by attending to things beyond the self. Although the universality of Maslow’s theory has been challenged, many believe it captures fundamental truths about human motivation.
Where does motivation come from?
Motivation can stem from a variety of sources. People may be motivated by external incentives, such as the motivation to work for compensation, or internal enjoyment, such as the motivation to create artwork in one’s spare time. Other sources of motivation include curiosity, autonomy, validation of one’s identity and beliefs, creating a positive self-image, and the desire to avoid potential losses.
Uses
There are many different uses for motivation. It serves as a guiding force for all human behavior, but understanding how it works and the factors that may impact it can be important in a number of ways.
Understanding motivation can:
Help improve the efficiency of people as they work toward goals
Help people take action
Encourage people to engage in health-oriented behaviors
Help people avoid unhealthy or maladaptive behaviors such as risk-taking and addiction
Help people feel more in control of their lives
Improve overall well-being and happiness
Impact
Anyone who has ever had a goal (like wanting to lose 20 pounds or run a marathon) probably immediately realizes that simply having the desire to accomplish something is not enough. Achieving such a goal requires the ability to persist through obstacles and endurance to keep going in spite of difficulties.
There are three major components of motivation: activation, persistence, and intensity.3
Activation involves the decision to initiate a behavior, such as enrolling in a psychology class.
Persistence is the continued effort toward a goal even though obstacles may exist. An example of persistence would be taking more psychology courses in order to earn a degree although it requires a significant investment of time, energy, and resources.
Intensity can be seen in the concentration and vigor that goes into pursuing a goal.4 For example, one student might coast by without much effort, while another student will study regularly, participate in discussions, and take advantage of research opportunities outside of class. The first student lacks intensity, while the second pursues their educational goals with greater intensity.
The degree of each of these components of motivation can impact whether or not you achieve your goal. Strong activation, for example, means that you are more likely to start pursuing a goal. Persistence and intensity will determine if you keep working toward that goal and how much effort you devote to reaching it.
Behavior
So how does motivation behave? With presence, intensity, and quality. Motivation is visible through gestures and facial expressions, intense effort, immediacy (or as psychologists like to call it short latency).
The presence of motivation can also be inferred from the levels of persistence and decisiveness in choosing one goal over another, which taken together make for a high probability of occurrence (Atkinson & Birch, 1970; 1978; Bolles, 1975; Ekman & Friesen, 1975).
Engagement
Motivation can also be inferred from the level of engagement.
For example, in a coaching scenario or a motivational interview, a competent practitioner will enthusiastically and generously contribute to the flow of conversation (agentic engagement), express interest and enjoyment (emotional engagement), process deeply and pay attention (cognitive engagement), and persist in these efforts as if time and the outside world didn’t exist (behavioral engagement). And yes, for many of us, we don’t have those kinds of conversations often.
Psychophysiology
There are five psychophysiological expressions of motivation:
Psychophysiological Expressions
Hormonal activity
Chemicals in saliva or blood, such as cortisol (stress) or catecholamines (fight-or-flight reaction).
Cardiovascular activity
Contraction and relaxation of the heart and blood vessels (as in response to an attractive incentive or a difficult/challenging task).
Ocular activity
Eye behavior—pupil size (extent of mental activity), eye blinks (changing cognitive states), and eye movements (reflective thought).
Electrodermal activity
Electrical changes on the surface of the skin (as in response to a significant or threatening event).
Skeletal activity
The activity of the musculature, as with facial expressions (specific emotion), bodily gestures, or shifting one’s weight from side to side during a boring hallway conversation (desire to leave).
Brain Activations
Just like changes in behavior, engagement, and psychophysiology, brain activations mark the rise and fall and maintenance of motivational states. A different pattern of neural activity is present with each motivation and emotion. For example, the hypothalamus is active when we are thirsty, and when we feel disgusted, there is a rise in insular activity.
Researchers use sophisticated equipment like electroencephalography (EEG) and functional magnetic resonance imaging (fMRI) to observe, detect, monitor, and measure brain-based neural activity.
See our blog post on Motivation Science for more information on the neuroscience of motivation.
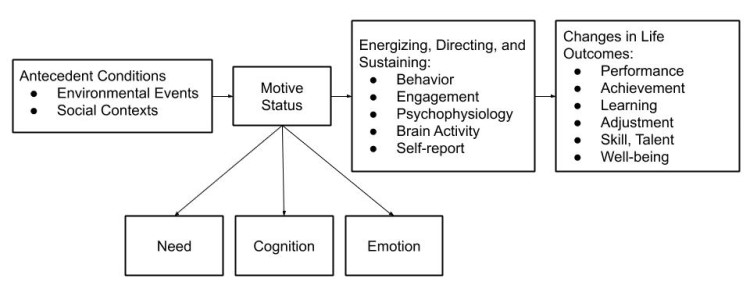
Putting all this together to answer the perennial question of what motivation is, but most importantly what it does, we define motivation as rising and falling of needs, cognition, and emotions expressed through patterns of behavior, levels of engagement and neural and psychophysiological activity directed toward realizing essential life outcomes.
Motivation Model
In a nutshell, motives are internal experiences in the form of needs, cognitions, and emotions and are the direct and proximal causes of motivated action. Social contexts and external events act as antecedents to motives that cause or trigger motivational states. Our motives express themselves through behavior, engagement, psychophysiology, brain activations, and self-report.
The model below illustrates the framework for how motivational psychologists study the process of motivation and its elements and try to find the answer to the questions about what causes motivation. It also shows why the study of motivation is so relevant to people’s lives and how motivation contributes positively to significant life outcomes like achievement, performance, and wellbeing, to name a few (Reeve, 2015).
Potential Pitfalls
There are a few things you should watch for that might hurt your motivation. These include:
Quick fixes or all-or-nothing thinking. It’s easy to feel unmotivated if you can’t fix something immediately or if you can’t have it all at once. Remind yourself that reaching your goals takes time.
Thinking that one size fits all. Just because an approach or method worked for someone else does not mean that it will work for you. If something isn’t helping you reach your goals or is making you feel unmotivated, look for things that will work better for you.
Motivation Process
Our motivation, when it originates from internal motives, as categorized into needs, cognitions, and emotions, is often experienced as more immediate and potent then extrinsic motivation.
Since we don’t exist in a vacuum, however, these inner experiences cannot take place without some degree of the external influence, be it in the form of consequences, incentives, or other forms of pressure arising out of the social context of our environment.
Our physiological and psychological needs drive us, our cognitions direct us, and emotions land intensity and energy to our pursuits. When the combination of antecedent conditions and the internal motives align, they create a ripe environment for engagement, which propels the action behavior.
When these behaviors, in turn, create more positive motivational and emotional states, they reinforce the behavior through a positive feedback loop and increase the likelihood of repetition.
The greatest thief this world has ever produced is procrastination, and he is still at large.
Josh Billings
Consider a motivational problem like procrastination or avoidance
Our needs, cognitions, emotions, environments, and relationships can play a crucial role in procrastination or avoidance.
All needs are born either out of deficiency or need for growth. Physiological needs are a particularly strong force in determining behavior. Our bodies will signal our brain if our wellbeing is threatened, and this can lead to avoidance and procrastination when we are suffering from hunger, thirst, or lack of sleep, for example.
Psychological needs are also significant drivers of motives as they represent inborn needs for the development of a sense of autonomy, competence, and relatedness. When we try to force ourselves to do something that contradicts those needs, these innate forces can be tough to overcome.
The conflict between chosen behavior and the need for satisfaction of psychological needs like autonomy can create dissonance, which can lead to avoidance or procrastination. While the fulfillment of physiological needs is about preserving wellbeing, satisfying psychological needs is about thriving and growing as a person
When we are no longer able to change a situation, we are challenged to change ourselves.
Viktor E. Frankl
There are also implicit needs which are acquired from our environment through socioemotional development. They vary from person to person as our experiences vary, and unlike inborn psychological needs, implicit motives are acquired.
Implicit here means unconscious. These needs occur without conscious awareness and are trait-like and enduring. Implicit needs motivate us toward the pursuit and attainment of specific social incentives (Schultheiss & Brunstein, 2010).
An implicit motive is a psychological need that arises from situational cues that cause emotional reactions, which then predict, guide, and explain people’s behavior and lifestyle. They can be inferred from the person’s characteristic thoughts, emotions, and behaviors. What a person “needs” within an implicit motive is to experience a particular pattern of affect or emotion.
For example, if we have little or no need for achievement, we may experience negative affect, such as anxiety, shame, and embarrassment while engaging in that challenging task and will avoid or procrastinate as a result. Implicit motives predict our behavior far more accurately than do explicit motives, which are basically what we tell others about what motives us (McClelland, Koestner, & Weinberger, 1989).
Our cognitions can also influence our tendency to avoid or procrastinate. Cognitions are mental constructs like goals, mindset, expectations, beliefs, and self-concept, to name a few that influence our motivation. If we have conflicting goals, for example, we may be more likely to avoid or procrastinate.
Change the way you look at things and the things you look at change.
Wayne W. Dyer
Emotions, although closely linked to cognitions and psychological needs, in and of themselves can motivate or demotivate. They can signal the importance of particular behavior. We may feel joy or pride at the possibility of goal attainment through engagement in particular behavior, or we can be afraid of failure and choose to avoid or procrastinate.
Our environment can also be either ideal and supportive or an obstacle to staying motivated and achieving our goals (Reeve, 2015). It can be full of distractions or lack optimal conditions that allow for sustained motivation.
Finally, our relationships can be supportive and empowering when it comes to change. This can be explained through a concept like the Michelangelo phenomenon, where our relationships support our potential. They can also be demotivating as in the Blueberry phenomenon, where the relationship brings out the worst in us and can contribute to procrastination and avoidance.
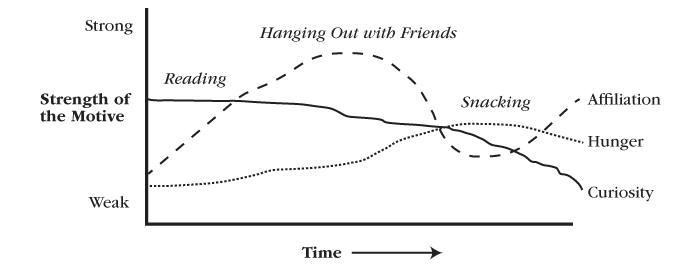
Motivation Cycle
Motivation is a dynamic process, and our motives vary over time. Raising and falling as circumstances change, and as time passes, motives contribute to the ongoing stream of behavior. To further complicate matters, we are driven by a multitude of different motives at any one point in time.
One motive, usually the one most situationally appropriate, will be strongest and dominate our attention while other motives will be subordinate and lie relatively dormant. Although typically the strongest motive will have the most considerable influence on our behavior, as circumstances change, each subordinate motive can become dominant.
The below example shows how a student’s motivation to read varies over time in strength, starting relatively strong then weakening when compared to the need to hang out with friends or to eat a snack (Reeve, 2015).
The awareness of how motivation varies over time is particularly important when it comes to goal setting.
When we differentiate the motivational and the performance-based advantages versus disadvantages for those who adopt a short-term goal, as in eating less than 2000 calories today, versus performers who adopt a long-term goal, as in losing 20 pounds this year, we must consider the type of activity they are engaging in before making recommendations.
Short term goals work better for uninteresting activities as they boost commitment by providing feedback on progress more often, which further reinforces the effort to persist (Reeve, 2015).
Motivation to perform routine or boring activities can be improved; however, by providing clarity of goals and choice in how to perform a task. Clarity and choice can fuel a sense of mastery and autonomy, and both, in combination, can increase overall motivation as they satisfy basic psychological needs.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
When it comes to interesting tasks, or as Mihaly Csíkszentmihályi (1990) calls them autotelic activities, long-term goals work better as they often provide for greater flexibility and more autonomy in how to pursue them. Short terms milestones can feel intrusive for interesting activities. Autotelic activities are already engaging, and we are often intrinsically motivated to perform them because they produce enjoyment. But most importantly, we are motivated to pursue them in the absence of external rewards or incentives.
′Autotelic′ is a word composed of two Greek roots: auto (self), and telos (goal). An autotelic activity is one we do for its own sake because to experience it is the main goal.
Mihaly Csíkszentmihályi
We also need to keep in mind that motivation to act on the goals is often higher when the goal is based in the near future, while far off goals do not create the tension of immediacy that would motivate us to act right away (Reeve, 2015).
To learn more about the types of motivation that exist, see our article on Motivation and What Really Drives Human Behavior.
You can also find many different approaches to increase motivation in the below list of self-help books published on the subject. Some are more philosophical, others biographical, and a few present recent research in motivation psychology.
Motivation Theories: Top 8 Theories of Motivation – Explained!
Some of the most important theories of motivation are as follows: 1. Maslow’s Need Hierarchy Theory 2. Herzberg’s Motivation Hygiene Theory 3. McClelland’s Need Theory 4. McGregor’s Participation Theory 5. Urwick’s Theory Z 6. Argyris’s Theory 7. Vroom’s Expectancy Theory 8. Porter and Lawler’s Expectancy Theory.
From the very beginning, when the human organisations were established, various thinkers have tried to find out the answer to what motivates people to work. Different approaches applied by them have resulted in a number of theories concerning motivation.
These are discussed in brief in that order.
1. Maslow’s Need Hierarchy Theory:
It is probably safe to say that the most well-known theory of motivation is Maslow’s need hierarchy theory Maslow’s theory is based on the human needs. Drawing chiefly on his clinical experience, he classified all human needs into a hierarchical manner from the lower to the higher order.
In essence, he believed that once a given level of need is satisfied, it no longer serves to motivate man. Then, the next higher level of need has to be activated in order to motivate the man. Maslow identified five levels in his need hierarchy as shown in figure 17.2.
These are now discussed one by one:
1. Physiological Needs:
These needs are basic to human life and, hence, include food, clothing, shelter, air, water and necessities of life. These needs relate to the survival and maintenance of human life. They exert tremendous influence on human behaviour. These needs are to be met first at least partly before higher level needs emerge. Once physiological needs are satisfied, they no longer motivate the man.
2. Safety Needs:
After satisfying the physiological needs, the next needs felt are called safety and security needs. These needs find expression in such desires as economic security and protection from physical dangers. Meeting these needs requires more money and, hence, the individual is prompted to work more. Like physiological needs, these become inactive once they are satisfied.
3. Social Needs:
Man is a social being. He is, therefore, interested in social interaction, companionship, belongingness, etc. It is this socialising and belongingness why individuals prefer to work in groups and especially older people go to work.
4. Esteem Needs:
These needs refer to self-esteem and self-respect. They include such needs which indicate self-confidence, achievement, competence, knowledge and independence. The fulfillment of esteem needs leads to self-confidence, strength and capability of being useful in the organisation. However, inability to fulfill these needs results in feeling like inferiority, weakness and helplessness.
5. Self-Actualisation Needs:
This level represents the culmination of all the lower, intermediate, and higher needs of human beings. In other words, the final step under the need hierarchy model is the need for self-actualization. This refers to fulfillment.
The term self-actualization was coined by Kurt Goldstein and means to become actualized in what one is potentially good at. In effect, self- actualization is the person’s motivation to transform perception of self into reality.
According to Maslow, the human needs follow a definite sequence of domination. The second need does not arise until the first is reasonably satisfied, and the third need does not emerge until the first two needs have been reasonably satisfied and it goes on. The other side of the need hierarchy is that human needs are unlimited. However, Maslow’s need hierarchy-theory is not without its detractors.
The main criticisms of the theory include the following:
1. The needs may or may not follow a definite hierarchical order. So to say, there may be overlapping in need hierarchy. For example, even if safety need is not satisfied, the social need may emerge.
2. The need priority model may not apply at all times in all places.
3. Researches show that man’s behaviour at any time is mostly guided by multiplicity of behaviour. Hence, Maslow’s preposition that one need is satisfied at one time is also of doubtful validity.
4. In case of some people, the level of motivation may be permanently lower. For example, a person suffering from chronic unemployment may remain satisfied for the rest of his life if only he/she can get enough food.
Notwithstanding, Maslow’s need hierarchy theory has received wide recognition, particularly among practicing managers. This can be attributed to the theory’s intuitive logic and easy to understand. One researcher came to the conclusion that theories that are intuitively strong die hard’.
2. Herzberg’s Motivation Hygiene Theory:
The psychologist Frederick Herzberg extended the work of Maslow and propsed a new motivation theory popularly known as Herzberg’s Motivation Hygiene (Two-Factor) Theory. Herzberg conducted a widely reported motivational study on 200 accountants and engineers employed by firms in and around Western Pennsylvania.
He asked these people to describe two important incidents at their jobs:
(1) When did you feel particularly good about your job, and
(2) When did you feel exceptionally bad about your job? He used the critical incident method of obtaining data.
The responses when analysed were found quite interesting and fairly consistent. The replies respondents gave when they felt good about their jobs were significantly different from the replies given when they felt bad. Reported good feelings were generally associated with job satisfaction, whereas bad feeling with job dissatisfaction. Herzberg labelled the job satisfiers motivators, and he called job dissatisfies hygiene or maintenance factors. Taken together, the motivators and hygiene factors have become known as Herzberg’s two-factor theory of motivation
Herzberg’s motivational and hygiene factors have been shown in the Table 17.1
According to Herzberg, the opposite of satisfaction is not dissatisfaction. The underlying reason, he says, is that removal of dissatisfying characteristics from a job does not necessarily make the job satisfying. He believes in the existence of a dual continuum. The opposite of ‘satisfaction’ is ‘no satisfaction’ and the opposite of ‘dissatisfaction’ is ‘no dissatisatisfaction’.
According to Herzberg, today’s motivators are tomorrow’s hygiene because the latter stop influencing the behaviour of persons when they get them. Accordingly, one’s hygiene may be the motivator of another.
However, Herzberg’s model is labeled with the following criticism also:
1. People generally tend to take credit themselves when things go well. They blame failure on the external environment.
2. The theory basically explains job satisfaction, not motivation.
3. Even job satisfaction is not measured on an overall basis. It is not unlikely that a person may dislike part of his/ her job, still thinks the job acceptable.
4. This theory neglects situational variable to motivate an individual.
Because of its ubiquitous nature, salary commonly shows up as a motivator as well as hygine.
Regardless of criticism, Herzberg’s ‘two-factor motivation theory’ has been widely read and a few managers seem untaminar with his recommendations. The main use of his recommendations lies in planning and controlling of employees work.
3. McClelland’s Need Theory:
Another well-known need-based theory of motivation, as opposed to hierarchy of needs of satisfaction-dissatisfaction, is the theory developed by McClelland and his associates’. McClelland developed his theory based on Henry Murray’s developed long list of motives and manifest needs used in his early studies of personality. McClelland’s need-theory is closely associated with learning theory, because he believed that needs are learned or acquired by the kinds of events people experienced in their environment and culture.
He found that people who acquire a particular need behave differently from those who do not have. His theory focuses on Murray’s three needs; achievement, power and affiliation. In the literature, these three needs are abbreviated “n Ach”, “n Pow”, and “n Aff” respectively’.
They are defined as follows:
Need for Achievement:
This is the drive to excel, to achieve in relation to a set of standard, and to strive to succeed. In other words, need for achievement is a behaviour directed toward competition with a standard of excellence. McClelland found that people with a high need for achievement perform better than those with a moderate or low need for achievement, and noted regional / national differences in achievement motivation.
Through his research, McClelland identified the following three characteristics of high-need achievers:
1. High-need achievers have a strong desire to assume personal responsibility for performing a task for finding a solution to a problem.
2. High-need achievers tend to set moderately difficult goals and take calculated risks.
3. High-need achievers have a strong desire for performance feedback.
Need for Power:
The need for power is concerned with making an impact on others, the desire to influence others, the urge to change people, and the desire to make a difference in life. People with a high need for power are people who like to be in control of people and events. This results in ultimate satisfaction to man.
People who have a high need for power are characterized by:
1. A desire to influence and direct somebody else.
2. A desire to exercise control over others.
3. A concern for maintaining leader-follower relations.
Need for Affiliation:
The need for affiliation is defined as a desire to establish and maintain friendly and warm relations with other people’. The need for affiliation, in many ways, is similar to Maslow’s social needs.
The people with high need for affiliation have these characteristics:
1. They have a strong desire for acceptance and approval from others.
2. They tend to conform to the wishes of those people whose friendship and companionship they value.
3. They value the feelings of others.
summary chart of the three need theories of motivation just discussed. The chart shows the parallel relationship between the needs in each of the theories. Maslow refers to higher- lower order needs, whereas Herzberg refers to motivation and hygiene factors.
4. McGregor’s Participation Theory:
Douglas McGregor formulated two distinct views of human being based on participation of workers. The first basically negative, labeled Theory X, and the other basically positive, labled Theory Y.
Theory X is based on the following assumptions:
1. People are by nature indolent. That is, they like to work as little as possible.
2. People lack ambition, dislike responsibility, and prefer to be directed by others.
3. People are inherently self-centered and indifferent to organisational needs and goals.
4. People are generally gullible and not very sharp and bright.
On the contrary,Theory Y assumes that:
1. People are not by nature passive or resistant to organisational goals.
2. They want to assume responsibility.
3. They want their organisation to succeed.
4. People are capable of directing their own behaviour.
5. They have need for achievement.
What McGregor tried to dramatise through his theory X and Y is to outline the extremes to draw the fencing within which the organisational man is usually seen to behave. The fact remains that no organisational man would actually belong either to theory X or theory Y. In reality, he/she shares the traits of both. What actually happens is that man swings from one set or properties to the other with changes in his mood and motives in changing .environment.
5. Urwick’s Theory Z:
Much after the propositions of theories X and Y by McGregor, the three theorists Urwick, Rangnekar, and Ouchi-propounded the third theory lebeled as Z theory.
The two propositions in Urwicks’s theory are that:
(i) Each individual should know the organisational goals precisely and the amount of contribution through his efforts towards these goals.
(ii) Each individual should also know that the relation of organisational goals is going to satisfy his/her needs positively.
In Urwick’s view, the above two make people ready to behave positively to accomplish both organisational and individual goals.
However, Ouchi’s Theory Z has attracted the lot of attention of management practitioners as well as researchers. It must be noted that Z does not stand for anything, is merely the last alphabet in the English Language.
Theory Z is based on the following four postulates:
1. Strong Bond between Organisation and Employees
2. Employee Participation and Involvement
3. No Formal Organisation Structure
4. Human Resource Development
Ouchi’s Theory Z represents the adoption of Japanese management practices (group decision making, social cohesion, job security, holistic concern for employees, etc.)by the American companies. In India, Maruti-Suzuki, Hero-Honda, etc., apply the postulates of theory Z.
6. Argyris’s Theory:
Argyris has developed his motivation theory based on proposition how management practices affect the individual behaviour and growth In his view, the seven changes taking place in an individual personality make him/her a mature one. In other words, personality of individual develops
Argyris views that immaturity exists in individuals mainly because of organisational setting and management practices such as task specialisation, chain of command, unity of direction, and span of management. In order to make individuals grow mature, he proposes gradual shift from the existing pyramidal organisation structure to humanistic system; from existing management system to the more flexible and participative management.
He states that such situation will satisfy not only their physiological and safety needs, but also will motivate them to make ready to make more use of their physiological and safety needs. But also will motivate them to make ready to make more use of their potential in accomplishing organisational goals.
7. Vroom’s Expectancy Theory:
One of the most widely accepted explanations of motivation is offered by Victor Vroom in his Expectancy Theory” It is a cognitive process theory of motivation. The theory is founded on the basic notions that people will be motivated to exert a high level of effort when they believe there are relationships between the effort they put forth, the performance they achieve, and the outcomes/ rewards they receive.
The relationships between notions of effort, performance, and reward are depicted in
Thus, the key constructs in the expectancy theory of motivation are:
1. Valence:
Valence, according to Vroom, means the value or strength one places on a particular outcome or reward.
2. Expectancy:
It relates efforts to performance.
3. Instrumentality:
By instrumentality, Vroom means, the belief that performance is related to rewards.
Thus, Vroom’s motivation can also be expressed in the form of an equation as follows: Motivation = Valence x Expectancy x Instrumentality
Being the model multiplicative in nature, all the three variables must have high positive values to imply motivated performance choice. If any one of the variables approaches to zero level, the possibility of the so motivated performance also touches zero level.
However, Vroom’s expectancy theory has its critics. The important ones are:
1. Critics like Porter and Lawler lebeled it as a theory of cognitive hedonism which proposes that individual cognitively chooses the course of action that leads to the greatest degree of pleasure or the smallest degree of pain.
2. The assumption that people are rational and calculating makes the theory idealistic.
3. The expectancy theory does not describe individual and situational differences.
But the valence or value people place on various rewards varies. For example, one employee prefers salary to benefits, whereas another person prefers to just the reverse. The valence for the same reward varies from situation to situation.
In spite of all these critics, the greatest point in me expectancy theory is that it explains why significant segment of workforce exerts low levels of efforts in carrying out job responsibilities.
8. Porter and Lawler’s Expectancy Theory:
In fact, Porter and Lawler’s theory is an improvement over Vroom’s expectancy theory. They posit that motivation does not equal satisfaction or performance. The model suggested by them encounters some of the simplistic traditional assumptions made about the positive relationship between satisfaction and performance. They proposed a multi-variate model to explain the complex relationship that exists between satisfaction and performance.
What is the main point in Porter and Lawler’s model is that effort or motivation does not lead directly to performance. It is intact, mediated by abilities and traits and by role perceptions. Ultimately, performance leads to satisfaction,. The same is depicted in the following
There are three main elements in this model. Let us briefly discuss these one by one.
Effort:
Effort refers to the amount of energy an employee exerts on a given task. How much effort an employee will put in a task is determined by two factors-
(i) Value of reward and
(ii) Perception of effort-reward probability.
Performance:
One’s effort leads to his/her performance. Both may be equal or may not be. However the amount of performance is determined by the amount of labour and the ability and role perception of the employee. Thus, if an employee possesses less ability and/or makes wrong role perception, his/her performance may be low in spite of his putting in great efforts.
Satisfaction:
Performance leads to satisfaction. The level of satisfaction depends upon the amount of rewards one achieves. If the amount of actual rewards meet or exceed perceived equitable rewards, the employee will feel satisfied. On the country, if actual rewards fall short of perceived ones, he/she will be dissatisfied.
Rewards may be of two kinds—intrinsic and extrinsic rewards. Examples of intrinsic rewards are such as sense of accomplishment and self-actualisation. As regards extrinsic rewards, these may include working conditions and status. A fair degree of research support that, the intrinsic rewards are much more likely to produce attitudes about satisfaction that are related to performance.
There is no denying of the fact that the motivation model proposed by Porter and Lawler is quite complex than other models of motivation. In fact motivation itself is not a simple cause-effect relationship rather it is a complex phenomenon Porter and Lawler have attempted to measure variables such as the values of possible rewards, the perception of effort-rewards probabilities and role perceptions in deriving satisfaction.
They recommended that the managers should carefully reassess their reward system and structure. The effort-performance-reward-satisfaction should be made integral to the entire system of managing men in organisation.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Maternal and perinatal mortality are still unacceptably high in many countries despite steep increases in facility birth. The evidence that childbirth in facilities reduces mortality is weak, mainly because of the scarcity of robust study designs and data. We aimed to assess this link by quantifying the influence of major determinants of facility birth (cluster-level facility birth, wealth, education, and distance to childbirth care) on several mortality outcomes, while also considering quality of care.
About 287 000 women died in 2010 of complications during pregnancy or childbirth. Most of these deaths can be avoided as the necessary medical interventions exist and are well known. The key obstacle is pregnant women’s lack of access to quality skilled care before, during and after childbirth.
Millennium Development Goal 5 (MDG 5), improve maternal health, set the targets of reducing maternal mortality by 75% and achieving universal access to reproductive health by 2015. But, so far progress in reducing maternal mortality in developing countries and providing family planning services has been too slow to meet the targets.
Causes of maternal mortality
The major direct causes of maternal morbidity and mortality include haemorrhage, infection, high blood pressure, unsafe abortion, and obstructed labour. These complications may arise unexpectedly. Investing in health systems – especially in training midwives and in making emergency obstetric care available round-the-clock – is key to reducing maternal mortality.
Addressing the barriers to use of care and creating a environment within households and community that support women in seeking the needed care is also key.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
The perinatal period
The perinatal period commences at 22 completed weeks (154 days) of gestation and ends seven completed days after birth. Perinatal and maternal health are closely linked.
Perinatal mortality refers to the number of stillbirths and deaths in the first week of life (early neonatal mortality).
In 2009 there were 2.6 million stillbirths globally with more than 8200 deaths a day. At least half of all stillbirths occurred in the intrapartum period. Among the 133 million babies born alive each year, 2.8 million die in the first week of life. The patterns of these deaths are similar to the patterns for maternal deaths; the majority occurring in developing countries. Quality skilled care during pregnancy and childbirth are key for the health of the baby and the mother.
WHO is supporting countries in delivering integrated, evidence-based and cost-effective care for mothers and babies that begins before conception and goes through pregnancy, childbirth and the postpartum period.
Methods
This paper draws on secondary data from 40 low and middle income countries that conducted emergency obstetric and newborn care assessments over the last 10 years. We reviewed 6.5 million deliveries, surveyed in 15,411 facilities. Most of the data were extracted from reports and aggregated with excel.
Results
Hemorrhage and hypertensive diseases contributed to about one third of institutional maternal deaths and indirect causes contributed another third (given the overrepresentation of sub-Saharan African countries with large proportions of indirect causes). The most lethal obstetric complication, across all regions, was ruptured uterus, followed by sepsis in Latin America and the Caribbean and sub-Saharan Africa. Stillbirth rates exceeded pre-discharge neonatal death rates in nearly all countries, possibly because women and their newborns were discharged soon after birth.
Conclusions
To a large extent, facility-based findings mirror what population-based systematic reviews have also documented. As coverage of a skilled attendant at birth increases, proportionally more deaths will occur in facilities, making improvements in record-keeping and health management information systems, especially for stillbirths and early neonatal deaths, all the more critical.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Puerperium is defined as the time from the delivery of the placenta through the first few weeks after the delivery. This period is usually considered to be 6 weeks in duration. By 6 weeks after delivery, most of the changes of pregnancy, labor, and delivery have resolved and the body has reverted to the nonpregnant state.
Puerperium, the period of adjustment after childbirth during which the mother’s reproductive system returns to its normal prepregnant state. It generally lasts six to eight weeks and ends with the first ovulation and the return of normal menstruation.
Puerperal changes begin almost immediately after delivery, triggered by a sharp drop in the levels of estrogen and progesterone produced by the placenta during pregnancy. The uterus shrinks back to its normal size and resumes its prebirth position by the sixth week. During this process, called involution, the excess muscle mass of the pregnant uterus is reduced, and the lining of the uterus (endometrium) is reestablished, usually by the third week. While the uterus returns to its normal condition, the breasts begin lactation. Colostrum, a high-protein form of milk, is produced by the second day after the birth and is gradually converted to normal breast milk, which has less protein and more fat, by the middle of the second week.
The chief medical problems associated with the puerperium include usually mild, transient depression, resulting from emotional letdown and discomfort associated with puerperal changes; clotting disorders, caused by blood stasis and prevented by an early return to normal activity; bleeding from a retained placenta; and puerperal fever, a major cause of maternal death until the 19th century. A combination of improved sanitary measures and modern antibiotics has now greatly reduced the mortality associated with puerperal fever.
Routine Postpartum Care
The immediate postpartum period most often occurs in the hospital setting, where the majority of women remain for approximately 2 days after a vaginal delivery and 3-4 days after a cesarean delivery. During this time, women are recovering from their delivery and are beginning to care for the newborn. This period is used to make sure the mother is stable and to educate her in the care of her baby (especially the first-time mother). While still in the hospital, the mother is monitored for blood loss, signs of infection, abnormal blood pressure, contraction of the uterus, and ability to void. There is also attention to Rh compatibility, maternal immunization statuses and breastfeeding.
Vaginal delivery
After a vaginal delivery, most women experience swelling of the perineum and consequent pain. This is intensified if the woman has had an episiotomy or a laceration. Routine care of this area includes ice applied to the perineum to reduce the swelling and to help with pain relief. Conventional treatment is to use ice for the first 24 hours after delivery and then switch to warm sitz baths. However, little evidence supports this method over other methods of postpartum perineum treatment. Pain medications are helpful both systemically as nonsteroidal anti-inflammatory drugs (NSAIDs) or narcotics and as local anesthetic spray to the perineum.
Hemorrhoids are another postpartum issue likely to affect women who have vaginal deliveries. Symptomatic relief is the best treatment during this immediate postpartum period because hemorrhoids often resolve as the perineum recovers. This can be achieved by the use of corticosteroid creams, witch hazel compresses, and local anesthetics in addition to a bowel regimen that avoids constipation.
Tampon use can be resumed when the patient is comfortable inserting the tampon and can maintain it without discomfort. This often takes longer for the woman who has had an episiotomy or a laceration than for one who has not. The vagina and perineum should first be fully healed, which takes several weeks. Tampons must be changed frequently to prevent infection.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Cesarean delivery
The woman who has had a cesarean delivery understandably will experience post-op pain at the abdominal incision. This, too, can be treated with heat or ice to the incision site, abdominal binder support, and use of systemic pain medication. Activities of daily living should be resumed as tolerated but without unnecessary delay.
Sexual intercourse
Sexual intercourse may resume when bright red bleeding ceases, the vagina and vulva are healed, and the woman is physically comfortable and emotionally ready. Physical readiness varies greatly among women but may take several weeks. Birth control is important to protect against pregnancy because the first ovulation is very unpredictable.
Patient education
Substantial education takes place during the hospital stay, especially for the first-time mother. The mother (and often the father) is taught routine care of the baby, including feeding, diapering, and bathing, as well as what can be expected from the baby in terms of sleep, urination, bowel movements, and eating.
Discharge instructions
The new mother should be given discharge instructions and expectations/precautions to consider once leaving the hospital. The most important information is who and where to call if she has problems or questions. She also needs details about resuming her normal activity. Instructions vary, depending on whether the mother has had a vaginal or a cesarean delivery and any comorbidities that may have been part of her care.
A systemic review of ovulation and menses in nonlactating women found that although most women begin ovulation at least 6 weeks postpartum, with mean day of first ovulation occurring 45-94 days postpartum, a limited number ovulate sooner.Two studies reporting earliest day of first ovulation reported it occurring on days 25 and 27 postpartum, emphasizing the need for early postpartum contraception discussion and method initiation to decrease the risk of pregnancy soon after delivery.
Many options are available, as follows:
Natural methods can be used in highly motivated couples, to include the use of monitoring the basal body temperature and the quality and quantity of the cervical mucus to determine what phase of the menstrual cycle the woman is in and if it is safe to have intercourse.
Barrier methods of contraception, such as condoms, are widely available, as are vaginal spermicides. Condoms are available over-the-counter, while diaphragms and cervical caps must be fitted.
Hormonal methods of contraception are numerous. Combined estrogen-progestin agents are taken daily by mouth or monthly by injection. Progestin-only agents are available for daily intake or by long-acting injections that are effective for 12 weeks.
Intrauterine devices can be placed immediately post partum (after delivery of the placenta) or after uterine involution occurs typically 4-6 weeks after delivery. Immediate postpartum insertion is associated with an increased risk of expulsion, approximately 24%. Immediate insertion is contraindicated in those with any postpartum infection including peripartum chorioamnionitis, endometritis or puerperal sepsis.
Permanent methods of birth control (ie, tubal ligation, vasectomy) are options for those who are certain they do not desire more children.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Liver disease that occurs during pregnancy can present a challenge for healthcare providers. Certain liver diseases are uniquely associated with pregnancy, whereas others are unrelated. The liver diseases unique to pregnancy include hyperemesis gravidarum, acute fatty liver of pregnancy (AFLP), intrahepatic cholestasis of pregnancy (ICP), and hemolysis and elevated liver enzymes and low platelets (HELLP) syndrome.Liver disease such as acute viral hepatitis can occur in pregnancy, and pregnancy may occur in a patient with underlying chronic liver disease, including patients with cirrhosis and portal hypertension, and patients who have undergone liver transplantation.
In the initial evaluation of a pregnant patient with abnormal liver tests, the American College of Gastroenterology (ACG) recommends these women undergo the same standard workup as that of nonpregnant individuals. With regard to imaging studies and/or endoscopy in pregnant women, the ACG has the following recommendations:
Ultrasonography is safe and the preferred imaging modality for the assessment of abnormal liver studies suggestive of biliary tract disease.
Magnetic resonance imaging (MRI) with gadolinium can be used in the second and third trimester.
Computed tomography (CT) scans carry a risk of teratogenesis and childhood hematologic malignancies but may be used judiciously with minimized radiation protocols (2-5 rads).
Endoscopy is safe in pregnancy but should be deferred until the second trimester if possible.
Meperidine and propofol can be used for endoscopic sedation.
Laboratory Value
Expected Trend in Pregnancy
Albumin
Decrease
Alkaline phosphatase
Increase
ALT
No expected change/slight decrease
AST
No expected change/slight decrease
Bilirubin
No expected change/slight decrease
Bile acid
No expected change
GGT
No expected change/slight decrease
Platelets
No expected change
Prothrombin time
No expected change
Modality
Pregnancy Considerations
Lactation Considerations
Other Issues
Ultrasound
Acceptable modality
Acceptable modality
No available data on contrasted ultrasound in pregnancy and lactation
CT
Risk of ionizing radiation exposure to fetus during pregnancy
Acceptable modality
Greatest risk of radiation exposure is at 8 to 15 weeks of gestation
Oral and iodinated contrast not teratogenic
Less than 1% of iodinated contrast is excreted in breast milk
MRI
Acceptable modality when performed without contrast
Acceptable modality with and without contrast
Gadolinium is associated with teratogenicity; crosses the placenta and is found in amniotic fluid and fetal circulation. Less than 0.04% is excreted into breast milk
Liver biopsy
Can be performed in pregnancy
Acceptable modality
Limited data on preterm births seen when performed during pregnancy
Upper endoscopy is acceptable in pregnancy and typically recommended to occur in the second trimester
Acceptable modality with consideration of compatibility of sedating medications with lactation
Ensure proper informed consent with discussion about fetal risks
Consideration of compatibility of sedating medications with pregnancy
Ensure adequate oxygenation and hemodynamic stability during procedure
Ensure left lateral decubitus position to avoid IVC compression
Liver Diseases That Are Unique to Pregnancy
Hyperemesis Gravidarum
Hyperemesis gravidarum (HG) is seen earlier than other liver diseases that are unique to pregnancy, typically presenting in the first trimester and resolving by the twentieth week of gestation. Occurring in about 0.3% to 2% of pregnancies, HG presents as intractable nausea and vomiting with subsequent dehydration, weight loss, electrolyte imbalance, and nutritional deficiency. Liver involvement is seen in 50% to 60% of patients with HG. Biochemical changes include elevations in aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels, which are typically mildly elevated but have been observed to rise to as high as 1,000 in some patients with HG. Jaundice is rare, occurring more commonly in severe cases of HG. The etiology of elevated liver enzymes in HG is unclear but has been proposed to involve liver cell injury due to multiple factors, including dehydration, starvation, and placental‐derived cytokines, including tumor necrosis factor alpha. It is noted that liver enzyme levels return to normal levels after resolution of HG, and thus there are no long‐term sequelae of HG on liver‐related health.
HG treatment involves administration of intravenous fluid, antiemetic therapy, and vitamin and mineral supplementation. Thiamine and folic acid supplementation are particularly emphasized, and metoclopramide, promethazine, and ondansetron are anti‐emetic therapies that are considered as compatible with pregnancy. Dietary modification should focus on consumption of small, frequent, low‐fat meals with high carbohydrate content. Enteral or parenteral nutrition can be cautiously considered in severe HG cases.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Hypertensive Disorders of Pregnancy
Hypertensive disorders of pregnancy that involve the liver include preeclampsia/eclampsia and the HELLP syndrome. Preeclampsia is seen in about 3% to 5% of pregnancies, and it is defined by the presence of new onset hypertension with a systolic blood pressure of ≥140 mm Hg and a diastolic blood pressure of ≥90 mm Hg measured on at least two occasions that are 4 to 6 hours apart and proteinuria of greater than 300 mg/day. Eclampsia occurs in about 1.4% of pregnancies; it is defined by the development of generalized seizures during preeclampsia. HELLP syndrome occurs in 0.2% to 0.6% of pregnancies and complicates 10% to 20% of cases of preelampsia/eclampsia. Whereas preeclampsia is typically described as occurring after the twentieth week of gestation, HELLP syndrome is predominantly considered as occurring in the third trimester between weeks 28 and 36 of gestation. In 30% of cases, HELLP syndrome presents in the early postpartum period.
HELLP syndrome has been viewed as representing one presentation on a spectrum of clinical manifestations of preeclampsia/eclampsia. Other manifestations of preeclampsia can involve hypertension in the absence of proteinuria, and in this clinical scenario, the presence of end‐organ injury in the setting of gestational hypertension can help to define preeclampsia. Due to the dilemma of distinguishing HELLP syndrome along the spectrum of preeclampsia/eclampsia, two diagnostic criteria for HELLP syndrome have been established. The Tennessee Classification categorizes HELLP syndrome as complete HELLP syndrome or partial HELLP syndrome, and the Mississippi Triple Class System divides HELLP syndrome into three classesBoth of these classification systems define subtypes of HELLP based on the severity of observed thrombocytopenia, liver enzyme elevations, and hemolysis.
HELLP Class
Mississippi Classification
Tennessee Classification
Class 1 (severe)
AST or ALT ≥70 IU/L
AST ≥70 IU/L
LDH ≥600 IU/L
LDH ≥600 IU/L or bilirubin ≥1.2 mg/dL
Platelet count ≤50 × 109/L
Class 2 (moderate)
AST or ALT ≥70 IU/L
N/A
LDH ≥600 IU/L
Platelet count 50‐100 × 109/L
Class 3 (mild)
AST or ALT ≥40 IU/L
N/A
LDH ≥600 IU/L
Platelet count 100‐150 × 109/L
Partial HELLP syndrome
Presence of severe preeclampsia plus one of the following: ELLP, EL, HEL, LP
Acute Fatty Liver of Pregnancy
Acute fatty liver of pregnancy (AFLP) is a rare disorder that occurs in about 1:7,000 to 1:15,000 pregnancies. Typically occurring in the third trimester, it involves maternal microvesicular fat deposition in the liver that leads to hepatic decompensation with potential for hepatic failure. Maternal mortality is 10% to 15%, and fetal mortality is up to 20%.
It is thought that AFLP is caused by inherited deficiencies of enzymes that are involved in the mitochondrial metabolism of fetal fatty acids. Impairment in fatty acid oxidation in the fetus and placenta can lead to increases in the levels of intermediate products of metabolism that accumulate in the placenta and maternal blood, leading to maternal hepatotoxicity. The most investigated fatty acid oxidation defect that is thought to contribute to AFLP is a deficiency in long chain 3‐hydroxyacyl‐coenzyme A‐dehydrogenase (LCHAD), which is a part of the mitochondrial trifunctional protein (MTP). G1528C and E474Q mutations of MTP are thought to be the cause of LCHAD deficiency and development of AFLP.
Coagulopathy (prothrombin time >14 seconds or activated partial thromboplastin time >34 seconds)
Radiographic features
Ascites or bright‐appearing liver on ultrasound
Histologic features
Microvesicular steatosis on liver biopsy
Intrahepatic Cholestasis of Pregnancy
Intrahepatic cholestasis of pregnancy (ICP) is the most common pregnancy‐related liver disease. Typically presenting in the second or third trimester of pregnancy, the prevalence of ICP is 0.1% to 2%. Epidemiologic data have indicated that it occurs with higher prevalence in South American and Scandinavian countries, and additional risk factors for it include advanced maternal age, multiparity, and a previous history of cholestasis with oral contraceptive use. The classic symptom of ICP is pruritus, but epigastric pain, fatigue, anorexia, and jaundice have also been observed. The typical laboratory finding in ICP is an elevation in bile acid levels. AST and ALT levels range from normal levels to 10 times to 20 times normal.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Pregnancy leads to physiologic changes in renal and systemic hemodynamics that cause important alterations in acid-base, electrolyte, and kidney function.
Understanding these changes is essential when evaluating pregnant women with kidney disease.
Disorders that cause acute kidney injury in early or late pregnancy generally fall into very different categories. It must also be remembered that pregnancies in women with underlying chronic kidney disease who require dialysis during pregnancy or who have previously undergone kidney transplantation pose unique sets of issues.
Ideally, women with kidney disease or systemic diseases that would put them at risk during pregnancy should receive preconception counseling from physicians knowledgeable about the current literature related to pregnancy. The team of physicians who care for these patients is often led by an experienced specialist in high-risk, maternal-fetal obstetrics working with a nephrologist and/or others. Successful maternal and fetal outcomes for women with preexisting kidney disease, and those with onset of kidney disease during pregnancy, require a close working relationship among all physicians involved in the care of these patients.
Overview of Acute Kidney Injury in Pregnancy
Acute kidney injury (AKI) is not common in pregnancy, and kidney injury requiring dialysis is very rare in pregnancy. Data from Canada reported an incidence of pregnancy-related AKI of 2.68 per 10,000 deliveries. AKI requiring dialysis in pregnancy or postpartum occur in 1 per 10,000 pregnant women, but it is associated with increased mortality.It is therefore important that clinicians who are asked to care for patients with this unusual complication be aware that while an acute reduction in GFR may result from any of the causes seen in the non-gravid state, a number of disorders are specific to pregnancy.
Pregnancy-specific kidney disorders generally can be organized into those occurring in early pregnancy and those occurring in late pregnancy.Disorders arising in early pregnancy include the following:
Prerenal azotemia
Acute tubular necrosis
Renal cortical necrosis
Pyelonephritis
Thrombotic thrombocytopenic purpura
Disorders arising in late pregnancy, almost all of which are usually specific to pregnancy, include the following:
Preeclampsia
Acute fatty liver of pregnancy
Hemolytic-uremic syndrome
The following conditions should also be considered in evaluating acute kidney injury in pregnancy:
Obstructive uropathy
Nephrolithiasis
Antiphospholipid syndrome
Obstructive uropathy should be considered in the setting of moderate or severe dilatation of the collecting system in women with oliguria or anuria. The most likely causes are the gravid uterus, polyhydramnios, kidney stones, and enlarged uterine fibroids. Obstructive uropathy usually resolves with delivery, although ureteral stenting may be required preterm.
In pregnancy, 1,25 di-hydroxycholecaliferol (vitamin D) levels are elevated due to increased production by the kidneys and placenta, resulting in hypercalciuria. This results in an increased risk of nephrolithiasis along with an increased risk of urinary tract infection. Ultrasonography is the primary diagnostic imaging modality used, and ureteral stenting may be necessary if the stones cannot be passed.
Women with anticardiolipin antibodies and the lupus anticoagulant are at risk of fetal loss and worsening renal function. All pregnant women with lupus should be screened for antiphospholipid antibodies and anti-Ro/SSA and anti-La/SSB antibodies. Treatment with low-dose aspirin or heparin should be considered but depends on the antibody levels, the risk of pre-eclampsia,and any previous obstetric history of early fetal loss and/or thrombosis.
Kidney Injury in Early Pregnancy
While prerenal azotemia can be caused by any cause of volume depletion during pregnancy, one of the more important causes is hyperemesis gravidarum. Hyperemesis gravidarum can be diagnosed by the history of persistent vomiting and is typically associated with metabolic alkalosis. Treatment consists of antiemetic therapy and volume replacement with intravenous normal saline and often potassium. Less commonly, hemorrhage associated with spontaneous abortion can also result in prerenal azotemia.
Acute tubular necrosis (ATN) in the first trimester is most likely to be caused by hemorrhage from spontaneous abortion or shock secondary to septic abortion. Septic abortion is most commonly due to gram-negative sepsis, primarily Escherichia coli, although in some cases, Clostridium perfringens is responsible, which can cause myonecrosis of the uterus and myoglobinuria. ATN due to these conditions is often more severe and more likely to require temporary dialysis until renal function recovers. ATN can also be caused by other causes seen in the non-gravid state, or by severe volume depletion from hyperemesis gravidarum.
The diagnosis of ATN should be suspected in the setting of septic abortion, and the diagnosis can be confirmed by urinalysis showing granular casts and urinary indices with an elevated fractional excretion of sodium. Treatment includes fluid resuscitation and pressors for hypotension; antibiotics; and, if necessary, dialysis.
Renal cortical necrosis (RCN) is a rare cause of severe AKI. RCN is more likely to be a cause of AKI in developing countries but even there, the incidence is falling. [9] Post-abortal sepsis is a common cause of RCN in developing countries, while abruptio placentae is responsible for RCN in 50%-60% of cases in pregnancy in developed countries. Other obstetric causes of RCN include puerperal sepsis, eclampsia, obstetric hemorrhage, intrauterine death, and thrombotic microangiopathy of pregnancy. Primary disseminated intravascular coagulation in the setting of severe renal ischemia is the most likely initiating event.
Postpartum Kidney Injury
Currently, most cases of AKI occur in the postpartum rather than the postabortal period, reflecting a decline in septic abortions and improvements in prenatal care. Postpartum AKI, TTP, and HUS represent overlapping syndromes that have in common severe hypertension, microangiopathic hemolytic anemia, thrombocytopenia, and AKI.
Patients with postpartum AKI usually present days to weeks following a normal delivery, with severe hypertension, hemolytic anemia, thrombocytopenia, and kidney failure. This disorder may also be related to retained placental fragments. HUS may be difficult to differentiate from severe preeclampsia or HELLP syndrome and may require postpartum kidney biopsy for diagnosis.
Kidney biopsy in HUS demonstrates glomerular thrombi and fibrin deposition, and fibrinoid necrosis of arterioles. When HUS is suspected, treatment should be initiated with plasma exchange or plasmapheresis. The value of corticosteroid therapy for HUS remains unclear.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Pregnancy and underlying kidney disease
In general, patients with chronic kidney disease (CKD) have reduced fertility. Only about 1.5% of women on long-term dialysis become pregnant. However, fertility improves significantly following kidney transplantation.
Historically, pregnancy has been regarded as posing very high risk to women with underlying kidney disease. However, the risk depends on the degree of kidney disease, the underlying disorder, and associated complications such as hypertension and proteinuria. It can therefore be difficult to predict the outcome in an individual patient.
Management of Kidney Disease in Pregnancy
Pregnant patients with kidney disease are often under the care of a maternal-fetal specialist who has advanced training in high-risk obstetrics. These patients receive frequent obstetric follow-up that includes careful blood pressure monitoring, renal function testing, and 24-hour urine protein collections. Consultation with a nephrologist often occurs, particularly for patients with more advanced disease and those with progressive renal failure.
Almost all patients with significant kidney disease and/or hypertension in late pregnancy, or when the likelihood of fetal viability is very high, are delivered and then can be managed as non-gravid patients. If progressive renal failure occurs either in early pregnancy or before fetal viability can be assured, however, dialysis may need to be considered.
Significant changes in dialysis care are required when managing a pregnant woman on hemodialysis. Nephrological management involves the intensification of dialysis dose, management of electrolytes, volume status, anemia, and bone care. Obstetric care concentrated on optimization and surveillance of fetal well-being and growth.
Dialysis should be initiated when the serum creatinine level is 3.5-5.0 mg/dL or the GFR is below 20 mL/min. Fetal outcome is improved with longer, more frequent hemodialysis sessions, which usually involves 20 hours of dialysis per week. Daily dialysis is more likely to prevent hypotension and significant metabolic shifts.
Dialysis should aim to keep BUN levels below 50 mg/dL, because controlling uremia may avoid polyhydramnios, control hypertension, and improve the mother’s nutritional status. Peritoneal dialysis with smaller volumes and frequent exchanges can also be done to achieve these same goals.
Anemia should be treated with erythropoietin-stimulating agents and careful attention to iron therapy. Nutritional support that allows weight gains of 0.3 to 0.5 kg/wk should be maintained in the second and third trimesters.
Pregnancy in patients receiving dialysis
Although fertility is significantly impaired in women with end-stage renal disease, pregnancy may still occur.Most women on dialysis are anovulatory, with either irregular or no menses, which can result in significant delays in the diagnosis of pregnancy in those who do conceive. In addition, the spontaneous abortion rate for pregnant women who require dialysis is approximately 50%. For pregnancies that continue, however, the fetal survival rate is as high as 71%.
Pregnancy in women with kidney transplants
Pregnancy in women following kidney transplantation has become commonplace. Transplantation restores fertility, and although most women with kidney transplants can deliver successfully, there is a higher risk of miscarriage, therapeutic abortion, stillbirth, ectopic pregnancy, preterm birth, low birthweight babies, and neonatal death.
Recommendations regarding health status for pregnancy in kidney transplant recipients include the following:
Good general health for 2 years post-transplantation, with serum creatinine levels below 2.0 mg/dL (preferably < 1.5 mg/dL)
No recent acute rejection or ongoing rejection
Normotension, or hypertension controlled with minimal antihypertensive agents
No or minimal proteinuria
No evidence of pelvicaliceal dilatation on renal ultrasonogram
Recommended immunosuppression in kidney transplant recipients includes the following:
Prednisone – Less than 15 mg per day (mg/d)
Azathioprine – 2 mg/kg/d or less
Calcineurin inhibitor–based therapy at appropriate therapeutic levels
Breast-feeding on cyclosporine is not recommended; tacrolimus may be taken during breast-feeding, though monitoring of infant levels is recommended.
Mycophenolate mofetil and sirolimus should be discontinued for 6 weeks prior to conception
If necessary, methylprednisolone is the preferred agent for treatment of rejection should it occur during pregnancy
The following are complication risks in kidney transplant recipients:
Immunosuppressive agents increase the risk of hypertension during pregnancy
Preeclampsia occurs in approximately one third of kidney transplant recipients
Almost 50% of pregnancies in these women end in preterm delivery due to hypertension
Blood levels of calcineurin inhibitors need to be frequently monitored due to changes in volumes of distribution of extracellular volume
There is an increased risk of cytomegalovirus, toxoplasmosis, and herpes infections, which raise concern for the fetus
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Life has lots of transitions — from infant to toddler, and youth to adult. For some, another transition is considering when to start a family.
Later in life, your transition may be to end fertility when you’re done growing your family.
If your next life transition involves birth control, you have some important choices to make. Depending on your stage of life, you may be considering either temporary or permanent birth control. Visit with your health care clinician or an OBGYN specialist about the best options for you.
Temporary Birth Control
Your options include:
Rhythm method — This involves not using birth control and avoiding sex during fertile times of the month.
Hormonal methods — Includes the pill, vaginal ring or a hormone patch. They mimic natural hormones in a woman’s body. They prevent ovulation and change the uterus and cervix so fertilization is much less likely to happen.
Barrier methods — Condoms, a diaphragm, sponge or cervical cap. The barriers stop sperm from reaching the egg.
Injectable methods — Progestin is injected every three months. Since the hormone dosage is less than other options, some patients prefer it. This method prevents conception similarly to other hormonal methods.
You may prefer a long-acting reversible contraceptive (LARC). These methods can last for three to 10 years. LARCs include:
Intrauterine devices — A T-shaped device is inserted into the uterus. The devices keep sperm from reaching the egg. There are two types of IUDs, hormonal and non-hormonal. Copper, non-hormone containing IUDs last approximately 10 years and hormone containing IUDSs last 3 to 5 years.
Hormonal implants — A match-stick sized plastic rod is implanted under the skin of the patient’s upper arm. The rod releases a special contraceptive hormone. This delivery system has hormonal results similar to hormonal and injectable methods.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Permanent Birth Control
Your health care clinician can give you important information about your options for permanent birth control — also known as sterilization. The National Institutes of Health describes three approaches:
Tubal ligation — During this surgery, the clinician cuts, ties or seals your fallopian tubes. This blocks the egg’s path from your ovaries to the uterus. It also stops sperm from reaching the egg.
Sterilization implant — This is a nonsurgical way to block your fallopian tubes. A clinician inserts a thin tube through the vagina and into the uterus. A soft, flexible implant is placed in each fallopian tube. During the following three months scar tissue forms around the implants. This scar tissue blocks the fallopian tubes so sperm can’t reach the egg. Temporary birth control is used while the fallopian tube tissue changes.
Vasectomy — This is an option for permanent male birth control. A surgeon cuts, closes or blocks the vas deferens. This is the duct that carries sperm from the testes to the ejaculatory ducts. Once the duct is blocked, sperm can’t leave the testis. This procedure may not be fully effective for up to three months. Temporary birth control is used during the three months after the procedure.
When considering permanent birth control options, check with your health care clinician. Some health care facilities have policies that limit the permanent birth control options they offer. Tubal ligation and vasectomy may not be available to you.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com