REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Congenital pseudarthrosis of the tibia (CPT) refers to nonunion of a tibial fracture that develops spontaneously or after a minor trauma. A pseudarthrosis is defined as a “false joint” and is a break in the bone that fails to heal on its own. The pseudarthrosis usually develops within the first two years of life; however, there have been reported cases of CPT development before birth as well as later in life.
Congenital pseudarthrosis of the tibia is a shin bone fracture in children that has not healed. It normally presents before a child turns two years old. Typically, the child gets a shin bone fracture that either happens spontaneously, or results from when the child experiences a minor trauma, and the fracture will not heal. It is a rare condition that occurs in 1 out of every 250,000 children.
It stems from the periosteum, a membrane that covers the bone, being abnormal and preventing proper bone healing. Since the bone has not healed correctly, it is unstable and there is mobility at the false joint which should be solid, stable bone. As a result, many patients have an unstable leg, making function difficult.

Classification Systems
Classification systems of CPT based on onset, mobility, and x-rays have been proposed. Difficulties of classification, however, have arisen because the condition includes different clinical and pathological entities each with a different history and prognosis. For example, classification systems based on the appearance of the tibia can become confusing since the appearance can change during treatment.
Dr. Paley, in conjunction with Dr. El-Rosassy, developed a classification system designed to indicate prognosis and treatment. The El-Rosassy-Paley classification system divides CPT into three types based on two criteria: the geometry of the bone ends and how mobile they are—that is, whether the bone ends at the pseudarthrosis are thick and stiff or thin and mobile. Another important consideration in the El-Rosassy-Paley classification is whether the patient has undergone a previous, unsuccessful surgery.
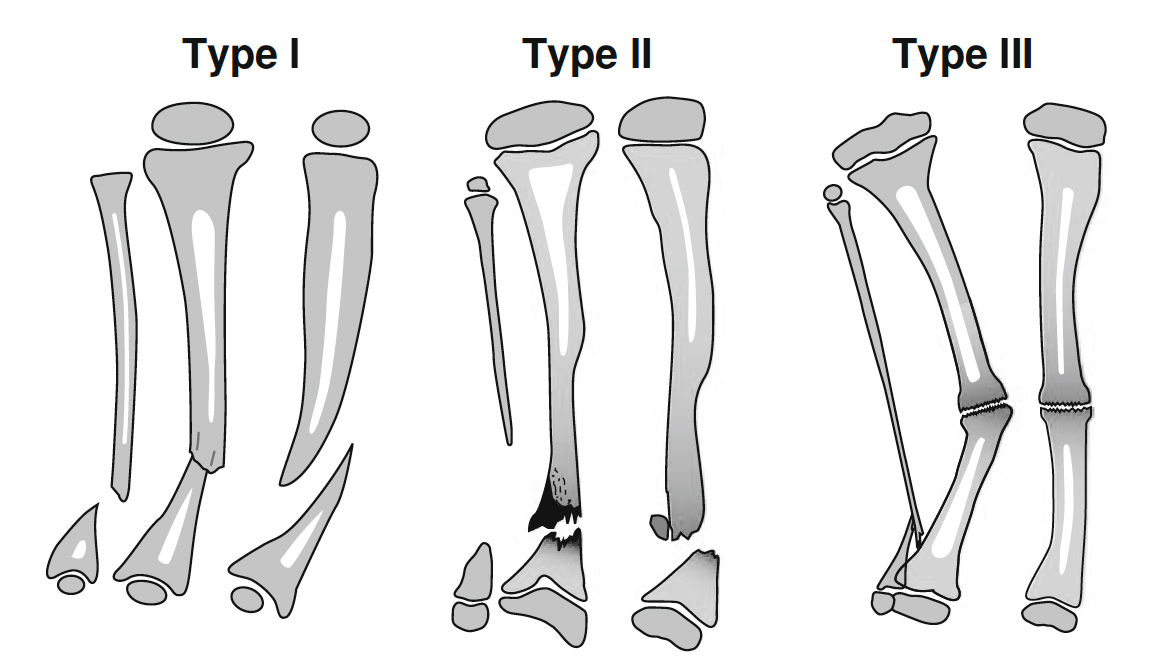
Type 1
- Atrophic (narrow) bone ends
- Mobile pseudarthrosis
- No previous surgery
Type 2
- Atrophic (narrow) bone ends
- Mobile pseudarthrosis
- Previous unsuccessful surgery
Type 3
- Hypertrophic (wide) bone ends
- Stiff pseudarthrosis
Congenital pseudarthrosis of the tibia remains one of the most challenging and misunderstood conditions in orthopedics. The difficulty of treatment lies in the weak healing power at the fracture site, a tendency to refracture after treatment, and the difficulty of stabilizing small osteoporotic bone fragments in small children. Even in cases where a union has been achieved, there is a difficulty in maintaining it. Frequently, the end result is a frustrated child and family who have been through multiple failed surgeries and remain with a limb that is short, deformed, and almost functionless. For this reason, many orthopedic surgeons recommend amputation, particularly after a third failed surgery.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
Who gets congenital pseudarthrosis of the tibia?
Congenital pseudarthrosis of the tibia is often associated with neurofibromatosis (NF-1) which has many other serious potential manifestations. However, congenital pseudarthrosis of the tibia is also seen in fibrous dysplasia, osteofibrous dysplasia and cleidocranial dysostosis. A significant percentage remain without a known cause (“idiopathic”).
How is congenital pseudarthrosis of the tibia diagnosed?
Congenital pseudarthrosis of the tibia is typically identified with X-rays and physical examination. Patients who are deemed high risk (e.g., patients with neurofibromatosis) may have screening X-rays performed in early childhood. In some cases, the first sign is a deformity in the leg or a fracture that occurred with minimal trauma.

What will happen during a clinic visit for congenital pseudarthrosis of the tibia?
The doctor will evaluate the patient for neurofibromatosis, a genetic disorder that causes tumors to form on nerve tissue which occurs in 40-50% of patients. The doctor will also ask for a history of previous fractures and examine the leg to determine the range of motion of the false joint. X-rays will be taken to determine the quality of the bone, the condition of the joints, the amount of limb length discrepancy and the severity of any bone abnormalities.
How is congenital pseudarthrosis of the tibia treated?
The primary treatment goal of congenital pseudarthrosis of the tibia is to achieve union of the shin bone (tibia) and to maintain that union. Treatment also addresses the resulting limb length discrepancies and bone deformities. To treat congenital pseudarthrosis of the tibia, the International Center for Limb Lengthening has a combined multimodal, comprehensive treatment program that addresses both the biological and mechanical issues. Many doctors use various elements of our protocol, but we strongly believe that the combined multimodal approach is the most effective.
What happens in surgery for congenital pseudarthrosis of the tibia?
- Two to four weeks before surgery, the patient receives a bisphosphonate infusion from our endocrinologist. Bisphosphonates inhibit cells responsible for breaking down bone. It is used to prevent resorption (melting away) of bone graft and to improve local healing response. This can take place in Baltimore or for patients from further away, it can be done closer to home by a local endocrinologist.
- In the operating room, the abnormal periosteum is removed from the tibia and fibula (both bones in the lower leg), and the pencil tip ends of the tibia and fibula are slightly trimmed to allow straightening of the leg with stable bone contact to optimize healing.
- The tibia is stabilized with intramedullary rods (inside the canal of the bone), and the fibula is stabilized with wires. Newer intramedullary rods have allowed surgeons to avoid crossing and damaging the ankle joint during fixation of almost all cases.
- Healthy periosteum and a bone graft are harvested from the pelvis usually on the same side as the tibia pseudarthrosis.
- The healthy periosteum, bone graft, and bone morphogenic protein (BMP) are placed in between and around the tibia and fibula bones, generating a large cross-sectional surface area for optimal healing. BMP is a naturally occurring cell signaling molecule that drives bone formation. When used in CPT treatment, it helps increase bone formation in the early stages. This is an off-label use of BMP in the United States (not approved by the FDA for this use). While healing can occur without BMP, it is an important component of the International Center for Limb Lengthening’s multi-faceted approach.
- In some cases, an external fixator is applied to the leg to provide rotational stability and to compress the bone ends while they knit. In most cases, an internal plate is used to control the newly realigned limb. In the past, external fixators were a necessity. The combination of the newer ankle-sparing intramedullary rods and improved internal plates gives surgeons another option to maintain improved ankle motion. Your doctor will assess which treatment is best for your child’s unique needs and circumstances.
- Once healing has occurred (typically evident by 2 months, and strong by 3-4 months), activity restrictions are lifted, and children can return to normal activities. A plastic leg brace called an ankle foot orthosis (AFO) is worn on the leg under clothing for additional protection.
- If an external fixator was used and healing of the tibia has been achieved, then the frame stays on for 3-4 months.
- If a proximal lengthening is being performed at the same time, then the frame is in place for 4-6 months. In the external fixation device, the patient is allowed to bear weight as soon as they would like after surgery. After the frame is removed, a long leg cast is placed for 4 weeks. After 4 weeks, the cast is removed and a brace is used for 2-3 months or longer.
- If a plate was used instead, the plate is removed 6-12 months after the initial surgery, while the rods remain inside to act as “rebar” to strengthen the newly healed leg and prevent refracture.
- After either method is used, regular monitoring of the bone is required on an annual basis. The internal rod may needs to be swapped out every 3-4 years during childhood as the leg grows longer to keep providing protection against refracture.
REQUEST AN APPOINTMENT OR BOOK A CONSULANT – Sargam.dange.18@gmail.com
